Welcome to the Afibber’s Forum
Serving Afibbers worldwide since 1999
Moderated by Shannon and Carey
 |
 |
 |
 |
 |
 |
Home
>
AFIBBERS FORUM
>
Topic
New to Afib and requesting high Potassium advice
Posted by MarkL
|
New to Afib and requesting high Potassium advice October 02, 2021 03:42PM |
Registered: 3 years ago Posts: 15 |
Just discovered this forum. Some great information here. Also am new to Afib. Let me say upfront that after doing some initial research (Google) I suspect it is unlikely I will discover a simple self-administered solution to this very complicated, multi-faceted condition. Also, I apologize up front for the long post.
I have a couple of questions I can’t seem to find the answer to anywhere, but first will give a little history to set the stage. I am 64 year old male (retired). Fairly active lifestyle. Have been a weightlifter since 1983 and an avid mountain biker of fairly technical singletrack trails since 1999. Battled familial hypertension since @ 1990. Around 3 years ago finally landed on the most successful BP meds combo to date that has well managed BP and HR. BP averages @ 110/70, resting HR @ 64. The stack is Telmisartan (Angiotensin Receptor Blocker), HCTZ(diuretic) and Carvedilol(beta blocker). Carvedilol keeps full exertion aerobic HR down to under 125 bpm.
Regarding diet, 2 years ago I started intermittent fasting by limiting all food intake daily and only eating from 6:00pm – 8:00pm in order to reduce lipids (familial again and am on a statin) and hopefully lower A1C which is on higher side of normal. Have followed this regimen very closely. Fast for 22 hours and then eat anything and everything like a starved maniac for 2 hours. Many of the foods are very high in potassium (meats, potatoes, high grain bread/brown rice, avocados, high K vegetables, etc). Once I adjusted to the fasting period I felt really good, had more energy, and significantly improved lipids (for me). Currently:
Total Cholesterol = 126
HDL = 38 – a little low but higher than my usual
LDL = 72
Triglycerides = 72
To note, other than recent onset of Afib events I have zero stress in my life. All was basically copasetic until mountain bike season really kicked in in early April this year. When I really started hitting it hard again was happily surprised to note that my cardio strength and stamina had significantly improved. By early May I increased my weekly 60 to 75 minute intense rides (as I had done for the past many years) from twice weekly up to three to four times weekly and my weight training from once per week to twice per week. By June 10 I started having episodes of racing heart that occurred ***ONLY *** after I went to bed @ 11:00pm. I had no chest pain, no dizziness, no fatigue, no chest pounding per se. The only way I can describe it is that I could feel some of the beats in my lower throat. I would get up and check my pulse rate via iphone apps and via manual wrist pulse check and could see the rate was all over the board from 42 to 130 BPM. It typically resolved on its own within 6 hours. Scary but figured it was a one-off and didn’t think that much about it until 2 weeks later when it hit again.
Early on I purchased a Kardia 6L and it indeed verified possible Afib. Below is a date list of the events I had. In all cases these occurred either upon going to bed before I fell alseep or could feel it upon arising in the morning and were verified by Kardia 6L. In almost all cases, they resolved without any intervention in @ 6 hours or less. Again, no negative symptoms other than racing heart. No reduction in exercise related cardio output, no pain or discomfort, etc.
Episode Dates
6/10/2021
6/24/2021
6/27/2021
7/11/2021
7/25/2021
7/31/2021
8/3/2021
8/12/2021
8/21/2021
8/23/2021
9/4/2021
9/23/2021
After a few of these I contacted my Internal Medicine Doctor (IMDoc) and sent her a few of the Kardia reports. Went in for exam, EKG normal (of course) and she could hear no mitral regurgitation. By this time I was pretty freaked about a stroke so she started me on Xarelto and ordered a Zio Patch. And yes, I am aware of the dangers of riding a mountain bike while on an anti-coagulant. Wore the patch for 2 weeks and it detected the events on 8/21 and 8/23. I had also felt those and captured them via Kardia. By @ 8/15 I had read (among many other things) the book “The Haywire Heart” and determined that I was most likely significantly overtraining. I immediately reduced weekly MTB rides back to 2 per week with a 10-minute break halfway through each ride and reduced weight training sessions to 1 per week.
Please bear with me I’m not to my questions yet. Since this all began in early June, I have (several times) on my own ordered a complete metabolic panel via Requestatest because I figured I was dehydrated. I had been taking some OTC potassium supplements once it started early on because I expected low potassium due to exercise heat induced dehydration. Much to my surprise my potassium levels were near the top of the scale from 4.9 to 5.2 even after I stopped supplementation. All other tests on the panel are almost exactly at the midpoint of their given ranges. Also, these tests were done after fasting for @ 18 to 20 hours. To note, during this time I eliminated almost all the typically reported triggers: stopped the occasional beer, reduced an already limited caffeine intake, made sure to sleep well and relax, increased daily water intake to at least 64 to 70 oz. and as mentioned have reduced exercise intensity and amount.
My Cardiologist is aware of all of this and has me scheduled for an echocardiogram in 3 weeks and then a follow-up appointment with her 3 weeks later. By then I should know for certain whether these are valve related. Had a standard protocol echo performed 2 years ago and it was fine. Hopefully it still is.
My first question is this: I have been reducing high potassium food for the past week. With my potassium being near the top of the range anyway, the fact that ARB’s are potassium sparing, and given the amount of food (lots of potassium) I eat during the 6:00 – 8:00 pm window, is it possible that I am spiking my serum potassium high enough to where @ 3 hours later when I go to bed and serum potassium from the meal might be peaking and my heart is fully relaxed, that this would all trigger paroxysmal Afib episodes?
I have read the Session document regarding potassium on this forum to the extent I could understand it but it seems to deal with low rather than high potassium and the balance of potassium, sodium and magnesium. It’s a little over my head. Both my IMDoc and Cardiologist say they don’t think my Afib events are related to high potassium or electrolytes. Cardiologist asked me to start “de-training” which I had already started.
My second question is this: Would it be beneficial at this point for me to get both a Potassium RBC and Magnesium RBC to see the intracellular values? And if so, is there anything I should look for other than “out of range”?
If you made it this far thanks for your time. Even if you don’t know the answers, any constructive comments based upon your personal experience/knowledge would be welcome & appreciated
Edited 3 time(s). Last edit at 10/03/2021 06:08PM by MarkL.
I have a couple of questions I can’t seem to find the answer to anywhere, but first will give a little history to set the stage. I am 64 year old male (retired). Fairly active lifestyle. Have been a weightlifter since 1983 and an avid mountain biker of fairly technical singletrack trails since 1999. Battled familial hypertension since @ 1990. Around 3 years ago finally landed on the most successful BP meds combo to date that has well managed BP and HR. BP averages @ 110/70, resting HR @ 64. The stack is Telmisartan (Angiotensin Receptor Blocker), HCTZ(diuretic) and Carvedilol(beta blocker). Carvedilol keeps full exertion aerobic HR down to under 125 bpm.
Regarding diet, 2 years ago I started intermittent fasting by limiting all food intake daily and only eating from 6:00pm – 8:00pm in order to reduce lipids (familial again and am on a statin) and hopefully lower A1C which is on higher side of normal. Have followed this regimen very closely. Fast for 22 hours and then eat anything and everything like a starved maniac for 2 hours. Many of the foods are very high in potassium (meats, potatoes, high grain bread/brown rice, avocados, high K vegetables, etc). Once I adjusted to the fasting period I felt really good, had more energy, and significantly improved lipids (for me). Currently:
Total Cholesterol = 126
HDL = 38 – a little low but higher than my usual
LDL = 72
Triglycerides = 72
To note, other than recent onset of Afib events I have zero stress in my life. All was basically copasetic until mountain bike season really kicked in in early April this year. When I really started hitting it hard again was happily surprised to note that my cardio strength and stamina had significantly improved. By early May I increased my weekly 60 to 75 minute intense rides (as I had done for the past many years) from twice weekly up to three to four times weekly and my weight training from once per week to twice per week. By June 10 I started having episodes of racing heart that occurred ***ONLY *** after I went to bed @ 11:00pm. I had no chest pain, no dizziness, no fatigue, no chest pounding per se. The only way I can describe it is that I could feel some of the beats in my lower throat. I would get up and check my pulse rate via iphone apps and via manual wrist pulse check and could see the rate was all over the board from 42 to 130 BPM. It typically resolved on its own within 6 hours. Scary but figured it was a one-off and didn’t think that much about it until 2 weeks later when it hit again.
Early on I purchased a Kardia 6L and it indeed verified possible Afib. Below is a date list of the events I had. In all cases these occurred either upon going to bed before I fell alseep or could feel it upon arising in the morning and were verified by Kardia 6L. In almost all cases, they resolved without any intervention in @ 6 hours or less. Again, no negative symptoms other than racing heart. No reduction in exercise related cardio output, no pain or discomfort, etc.
Episode Dates
6/10/2021
6/24/2021
6/27/2021
7/11/2021
7/25/2021
7/31/2021
8/3/2021
8/12/2021
8/21/2021
8/23/2021
9/4/2021
9/23/2021
After a few of these I contacted my Internal Medicine Doctor (IMDoc) and sent her a few of the Kardia reports. Went in for exam, EKG normal (of course) and she could hear no mitral regurgitation. By this time I was pretty freaked about a stroke so she started me on Xarelto and ordered a Zio Patch. And yes, I am aware of the dangers of riding a mountain bike while on an anti-coagulant. Wore the patch for 2 weeks and it detected the events on 8/21 and 8/23. I had also felt those and captured them via Kardia. By @ 8/15 I had read (among many other things) the book “The Haywire Heart” and determined that I was most likely significantly overtraining. I immediately reduced weekly MTB rides back to 2 per week with a 10-minute break halfway through each ride and reduced weight training sessions to 1 per week.
Please bear with me I’m not to my questions yet. Since this all began in early June, I have (several times) on my own ordered a complete metabolic panel via Requestatest because I figured I was dehydrated. I had been taking some OTC potassium supplements once it started early on because I expected low potassium due to exercise heat induced dehydration. Much to my surprise my potassium levels were near the top of the scale from 4.9 to 5.2 even after I stopped supplementation. All other tests on the panel are almost exactly at the midpoint of their given ranges. Also, these tests were done after fasting for @ 18 to 20 hours. To note, during this time I eliminated almost all the typically reported triggers: stopped the occasional beer, reduced an already limited caffeine intake, made sure to sleep well and relax, increased daily water intake to at least 64 to 70 oz. and as mentioned have reduced exercise intensity and amount.
My Cardiologist is aware of all of this and has me scheduled for an echocardiogram in 3 weeks and then a follow-up appointment with her 3 weeks later. By then I should know for certain whether these are valve related. Had a standard protocol echo performed 2 years ago and it was fine. Hopefully it still is.
My first question is this: I have been reducing high potassium food for the past week. With my potassium being near the top of the range anyway, the fact that ARB’s are potassium sparing, and given the amount of food (lots of potassium) I eat during the 6:00 – 8:00 pm window, is it possible that I am spiking my serum potassium high enough to where @ 3 hours later when I go to bed and serum potassium from the meal might be peaking and my heart is fully relaxed, that this would all trigger paroxysmal Afib episodes?
I have read the Session document regarding potassium on this forum to the extent I could understand it but it seems to deal with low rather than high potassium and the balance of potassium, sodium and magnesium. It’s a little over my head. Both my IMDoc and Cardiologist say they don’t think my Afib events are related to high potassium or electrolytes. Cardiologist asked me to start “de-training” which I had already started.
My second question is this: Would it be beneficial at this point for me to get both a Potassium RBC and Magnesium RBC to see the intracellular values? And if so, is there anything I should look for other than “out of range”?
If you made it this far thanks for your time. Even if you don’t know the answers, any constructive comments based upon your personal experience/knowledge would be welcome & appreciated
Edited 3 time(s). Last edit at 10/03/2021 06:08PM by MarkL.
|
Re: New to Afib and requesting high Potassium advice October 03, 2021 12:39AM |
Registered: 7 years ago Posts: 850 |
|
Re: New to Afib and requesting high Potassium advice October 03, 2021 02:55AM |
Registered: 3 years ago Posts: 15 |
Thanks Joe. Sodium typically hangs right at 138. Probably because of the HCTZ. Given that, I would have thought it would be keeping my potassium lower also. However, with a many year history of treatment for hypertension, I have always tried to limit sodium intake and increase potassium intake.
|
Re: New to Afib and requesting high Potassium advice October 03, 2021 01:04PM |
Registered: 12 years ago Posts: 4,534 |
Hi Mark,
I'll relate my experience. I'm 66 and my path to afib 17 years ago was chronic fitness. My first episode was about two days after a training run on a 14,000' peak - woke up with it. After two months of getting afib every 10-14 days, lasting 6-9 hours, I had an episode that would not convert. My EP suggested staying out of rhythm as my afib heart rate was low. I told him I had a "Plan B." At the time, I was winging it, but basically my plan was based on electrolytes and detraining.
What I learned for me is that my exercise trigger is the product of duration times intensity. Meaning I could do long duration activities at a moderate level. I empirically determined that this level was what researcher and head coach of the winning Tour de France team in 2020 and 2021, Iñigo San Millân, calls Zone 2. This is very well explained in this Peter Attia podcast with Iñigo. There are a couple of other approaches that approximate this intensity. Phil Maffetone's MAF method and always nasal breathing. I've linked these in this post. Exercise and afib is explored in this thread on the book, "The Haywire Heart."
I've learned I can do very high intensity training for very short durations. Currently I have a protocol that I do on a old Schwinn Airdyne Fan bike. It is 3 minutes mild at 50 watts, then 20 seconds at absolute maximum which is usually close to 800 watts (which I can only hold for a few seconds), then 3 minutes at 50, another max 20 and 3 minutes 20 seconds of 50 watts cool down.
The other piece is electrolytes. This evolved to magnesium to bowel tolerance, 4 g of ;potassium as citrate powder sipped over the day in a liter of water, 1/4- 1/2 tsp of taurine powder and keeping calcium low.
This combination has allowed me to keep afib episodes to a few episodes a year for all these years. When I do get afib, I generally take a loading dose of flecainide to convert (in my case 300 mg, if you weigh under 154 #/70kg the max dose is 200 mg). Otherwise, I take no meds, for afib or anything else. I also never exercise while in afib.
In your case, the meds obviously change the potassium equation. If your afib only occurs at 11 PM, perhaps moving your eating window earlier in the day - midday or morning. The 11PM time indicates a vagal trigger. Generally during the waking hours, this trigger would be less likely to raise its head. Also an earlier eating window would allow you to test serum potassium in a serial fashion, say every hour for four or five hours after your meal to see what is happening. Absent the meds, normal kidneys will excrete a bolus of potassium quickly.
My personal bias is to try to solve medical issues without meds whenever possible. When my BP started to increase, I used non pharma approaches to get it where it typically is 100-110/55-65. I have a genetic allele (ApoE4) that will raise my LDL, but my doc has a different view, so we worry about inflammation rather than trying to reduce it with meds. I eat a low glycemic whole foods diet that I prepare from scratch.
I'll relate my experience. I'm 66 and my path to afib 17 years ago was chronic fitness. My first episode was about two days after a training run on a 14,000' peak - woke up with it. After two months of getting afib every 10-14 days, lasting 6-9 hours, I had an episode that would not convert. My EP suggested staying out of rhythm as my afib heart rate was low. I told him I had a "Plan B." At the time, I was winging it, but basically my plan was based on electrolytes and detraining.
What I learned for me is that my exercise trigger is the product of duration times intensity. Meaning I could do long duration activities at a moderate level. I empirically determined that this level was what researcher and head coach of the winning Tour de France team in 2020 and 2021, Iñigo San Millân, calls Zone 2. This is very well explained in this Peter Attia podcast with Iñigo. There are a couple of other approaches that approximate this intensity. Phil Maffetone's MAF method and always nasal breathing. I've linked these in this post. Exercise and afib is explored in this thread on the book, "The Haywire Heart."
I've learned I can do very high intensity training for very short durations. Currently I have a protocol that I do on a old Schwinn Airdyne Fan bike. It is 3 minutes mild at 50 watts, then 20 seconds at absolute maximum which is usually close to 800 watts (which I can only hold for a few seconds), then 3 minutes at 50, another max 20 and 3 minutes 20 seconds of 50 watts cool down.
The other piece is electrolytes. This evolved to magnesium to bowel tolerance, 4 g of ;potassium as citrate powder sipped over the day in a liter of water, 1/4- 1/2 tsp of taurine powder and keeping calcium low.
This combination has allowed me to keep afib episodes to a few episodes a year for all these years. When I do get afib, I generally take a loading dose of flecainide to convert (in my case 300 mg, if you weigh under 154 #/70kg the max dose is 200 mg). Otherwise, I take no meds, for afib or anything else. I also never exercise while in afib.
In your case, the meds obviously change the potassium equation. If your afib only occurs at 11 PM, perhaps moving your eating window earlier in the day - midday or morning. The 11PM time indicates a vagal trigger. Generally during the waking hours, this trigger would be less likely to raise its head. Also an earlier eating window would allow you to test serum potassium in a serial fashion, say every hour for four or five hours after your meal to see what is happening. Absent the meds, normal kidneys will excrete a bolus of potassium quickly.
My personal bias is to try to solve medical issues without meds whenever possible. When my BP started to increase, I used non pharma approaches to get it where it typically is 100-110/55-65. I have a genetic allele (ApoE4) that will raise my LDL, but my doc has a different view, so we worry about inflammation rather than trying to reduce it with meds. I eat a low glycemic whole foods diet that I prepare from scratch.
|
Re: New to Afib and requesting high Potassium advice October 03, 2021 03:13PM |
Registered: 3 years ago Posts: 15 |
George thank you for the information and your insight. Early on, I didn’t really think about the over-training aspect until I read “The Haywire Heart”. It may not be the whole puzzle for me but probably has to be a significant part of it due to the fact that this didn’t start until I basically doubled the amount of training I was doing this time last year. I was just amazed and ecstatic that my cardio strength/stamina had improved so much. I’ve always been OCD regarding training and this enhanced ability fit like a glove into my psyche. Since I’m retired, I could easily incorporate the additional time necessary to double my training.
While I don’t and have never considered myself an “athlete” (more of an intense weekend warrior), my mountain biking rides typically consist of 60 to 75 minute sessions with no rest during that period. And many times I was trying to beat my best previous ride time for that particular trail. At least that’s what I was doing until @ 1 month ago. Mountain biking is (for me) the perfect fit for “interval training”. However, when I analyze it I, I am doing it backwards so to speak. The way I was riding consists of riding up a technical singletrack trail hills at FULL exertion for @ 15 to 30 seconds or longer and then relaxing/coasting down the other side before pedaling at full steam again to get up the next hill go down the other side. As you also know and proved from you current training, with true interval training it should be short full steam bursts followed by a much longer rest period. My riding is unfortunately the complete opposite of that. Rest periods have not been longer than the full steam effort time. I think your intensity times duration has to be a key factor. I have seen references to the Zone 2 training and will definitely pursue that research. Thank you much for the links. I recently have modified my sessions to cease riding to beat previous times and ride more for the fun of it. Also, I now stop at 30 minutes and take a full 10 minute rest before restarting my ride and stop again in 30 mins to rest again if the ride goes past that. Still not really interval training but at least it’s more rest than I was getting before.
Regarding electrolytes, that is currently a big black hole for me. Early on I thought my problem was related to dehydration/low potassium. Have always taken 400 mg Magnesium daily but suspected my Potassium was going low so I supplemented that and started Taurine. Once I did that it seems to have kicked my episodes into high gear and continued if not increased. That’s when I started having the CMP blood work done and was surprised to see potassium so high. Even after stopping the potassium and taurine supplements it remains on the upper end of the spectrum, ergo my question regarding how quickly serum potassium levels rise and can they rise quickly into a danger zone.
Regarding diet, I’ve decided, regardless of my potassium levels, it make NO sense whatsoever to eat the volume of food I am eating and then going to bed 3 hours later with a full stomach and sometimes bloated. Can’t be healthy for my heart strain or vagus nerve pressure, so that’s changing as of today. Yeah “maybe” it significantly improved my lipids but any benefit I gained there is certainly destroyed if it is going to induce afib. Plan to eat 2 smaller meals daily with the second meal finished by 6:30 pm.
Sounds like you are doing great and I’m glad you’ve found solutions that have worked. That’s my goal. Thanks again and take care.
While I don’t and have never considered myself an “athlete” (more of an intense weekend warrior), my mountain biking rides typically consist of 60 to 75 minute sessions with no rest during that period. And many times I was trying to beat my best previous ride time for that particular trail. At least that’s what I was doing until @ 1 month ago. Mountain biking is (for me) the perfect fit for “interval training”. However, when I analyze it I, I am doing it backwards so to speak. The way I was riding consists of riding up a technical singletrack trail hills at FULL exertion for @ 15 to 30 seconds or longer and then relaxing/coasting down the other side before pedaling at full steam again to get up the next hill go down the other side. As you also know and proved from you current training, with true interval training it should be short full steam bursts followed by a much longer rest period. My riding is unfortunately the complete opposite of that. Rest periods have not been longer than the full steam effort time. I think your intensity times duration has to be a key factor. I have seen references to the Zone 2 training and will definitely pursue that research. Thank you much for the links. I recently have modified my sessions to cease riding to beat previous times and ride more for the fun of it. Also, I now stop at 30 minutes and take a full 10 minute rest before restarting my ride and stop again in 30 mins to rest again if the ride goes past that. Still not really interval training but at least it’s more rest than I was getting before.
Regarding electrolytes, that is currently a big black hole for me. Early on I thought my problem was related to dehydration/low potassium. Have always taken 400 mg Magnesium daily but suspected my Potassium was going low so I supplemented that and started Taurine. Once I did that it seems to have kicked my episodes into high gear and continued if not increased. That’s when I started having the CMP blood work done and was surprised to see potassium so high. Even after stopping the potassium and taurine supplements it remains on the upper end of the spectrum, ergo my question regarding how quickly serum potassium levels rise and can they rise quickly into a danger zone.
Regarding diet, I’ve decided, regardless of my potassium levels, it make NO sense whatsoever to eat the volume of food I am eating and then going to bed 3 hours later with a full stomach and sometimes bloated. Can’t be healthy for my heart strain or vagus nerve pressure, so that’s changing as of today. Yeah “maybe” it significantly improved my lipids but any benefit I gained there is certainly destroyed if it is going to induce afib. Plan to eat 2 smaller meals daily with the second meal finished by 6:30 pm.
Sounds like you are doing great and I’m glad you’ve found solutions that have worked. That’s my goal. Thanks again and take care.
|
Re: New to Afib and requesting high Potassium advice October 03, 2021 04:07PM |
Registered: 12 years ago Posts: 4,534 |
Mark,
Some more observations.
- I learned early on that competing was a bad plan for me (whether with myself or others). My son always wanted me to go to CrossFit class with him and I would not do it as I knew I'd want to complete with him and the others - which would be counterproductive for my afib.
- One of the things I do that could be like your bike riding is alpine skiing the steeps off piste. I can do this all day long without issue, if I approach it in a relatively casual fashion. One day, 9 years ago, I decided to see how many gnarly runs I could do in a day. For an old guy, I racked up a bunch of vertical on this stuff. Bad plan. Afib was the later result. In a similar vein, was skiing the steeps on a lovely powder day. Decided to add hiking for more vertical to each lap, again, the hiking was a bad plan. I have a friend, 30 years younger, who commonly skins (hikes) up and skis down for a few laps in the morning. I don't join as the hiking up is a bad plan for me. I can rock climb all day without issue. Even when it is hard, it is generally burning out my muscles isometrically.
- I used to do "regular" Tabatas on the Schwinn bike (20 seconds as hard as possible and 10 seconds rest) for 8 reps. While this never was a delayed afib trigger, I commonly wear a Polar heart rate strap and record beat to beat data. In the beat to beat (r to r), I can see both PAC's and PVC's. Doing this program, I could see a lot of ectopics. With my two 20 second high intensity rounds in 10 minutes, my heart rate data are much "cleaner" with few ectopics. I also only do my 10 minute program two to three times per week. For the high intensity portion, I'm staying in the creatine phosphate energy system and in the aerobic - almost exclusively using fat for the rest periods (and same for Zone 2). I avoid engaging the anaerobic glycolytic systems as I hypothesize this is where the metabolic stress comes from that encourages afib.
- I've made strength training, cathistenics, isometrics & etc a Zone 2 project for me also.
- "Cardio" is all Zone 2, much of which I now do as Heavy Hands walking, or more generally trying to use as many muscles as possible, but wearing a heart rate monitor to keep in Z2. My next project is to get a lactate meter so I can dial in the Z2 better (keeping serum lactate between 1.5 & 2.0 mmol/L for Z2).
Some more observations.
- I learned early on that competing was a bad plan for me (whether with myself or others). My son always wanted me to go to CrossFit class with him and I would not do it as I knew I'd want to complete with him and the others - which would be counterproductive for my afib.
- One of the things I do that could be like your bike riding is alpine skiing the steeps off piste. I can do this all day long without issue, if I approach it in a relatively casual fashion. One day, 9 years ago, I decided to see how many gnarly runs I could do in a day. For an old guy, I racked up a bunch of vertical on this stuff. Bad plan. Afib was the later result. In a similar vein, was skiing the steeps on a lovely powder day. Decided to add hiking for more vertical to each lap, again, the hiking was a bad plan. I have a friend, 30 years younger, who commonly skins (hikes) up and skis down for a few laps in the morning. I don't join as the hiking up is a bad plan for me. I can rock climb all day without issue. Even when it is hard, it is generally burning out my muscles isometrically.
- I used to do "regular" Tabatas on the Schwinn bike (20 seconds as hard as possible and 10 seconds rest) for 8 reps. While this never was a delayed afib trigger, I commonly wear a Polar heart rate strap and record beat to beat data. In the beat to beat (r to r), I can see both PAC's and PVC's. Doing this program, I could see a lot of ectopics. With my two 20 second high intensity rounds in 10 minutes, my heart rate data are much "cleaner" with few ectopics. I also only do my 10 minute program two to three times per week. For the high intensity portion, I'm staying in the creatine phosphate energy system and in the aerobic - almost exclusively using fat for the rest periods (and same for Zone 2). I avoid engaging the anaerobic glycolytic systems as I hypothesize this is where the metabolic stress comes from that encourages afib.
- I've made strength training, cathistenics, isometrics & etc a Zone 2 project for me also.
- "Cardio" is all Zone 2, much of which I now do as Heavy Hands walking, or more generally trying to use as many muscles as possible, but wearing a heart rate monitor to keep in Z2. My next project is to get a lactate meter so I can dial in the Z2 better (keeping serum lactate between 1.5 & 2.0 mmol/L for Z2).
|
Re: New to Afib and requesting high Potassium advice October 03, 2021 05:42PM |
Registered: 3 years ago Posts: 15 |
George, thanks for the additional information. At this point most of what you are discussing is way over my pay grade of knowledge but I am in learning mode going forward. However, after reading your info above, I just read this on a MTB fitness website:
"There are three different energy systems that are used in any activity (including mountain biking). They are the aerobic, glycolytic, and the ATP systems. All of these systems are used, all of the time. But how much any one system is used depends on the duration and intensity of the activity."
Obviously, you already know this but again it does point to your duration times intensity experience.
For the past 5 years, single-track mountain biking has been the all time single most enjoyable fitness activity in my life. Can't do a lot of the things I did years ago like heavy weight lifting and racquetball due to several injuries and subsequent shoulder surgeries. As I mentioned, as of late I have reduced weekly number of rides, riding intensity, and am taking more breaks. My hope is changing my diet to smaller multiple meals and the reduction in riding intensity will be enough. However, even if this were to work, I have no idea how long it would take that to trend in reduced episodes. No clue what the turn around of improvements is.
Not bragging but many times when I am on the trails and I see a guy near my age (which is rare) and if I do he is riding an E-assisted MTB. On those you can pedal the heavier bike as much as you want manually but can use the battery assistance anytime you feel you need it. I have always taken pride that I was still climbing these hills manually at my age. But in thinking about it recently maybe they are simply MUCH smarter than me. They are not cheap bikes but light years cheaper than a stroke or MI. If that is the route I have to go to continue to ride AND reduce the risk of Afib then I am ready pursue that route.
Up until the past couple of months I simply refused to believe it could be the amount of biking I was doing. That was a combination of my ignorance of the Afib topic and the fact that my endurance had actually increased AND the fact that these episodes have NEVER occurred the night of a mountain bike ride earlier in the day. Turns out any of the contributing factors can have a cumulative and delayed onset which make its more difficult to try to self diagnose.
Anyway, thank you for your info.
"There are three different energy systems that are used in any activity (including mountain biking). They are the aerobic, glycolytic, and the ATP systems. All of these systems are used, all of the time. But how much any one system is used depends on the duration and intensity of the activity."
Obviously, you already know this but again it does point to your duration times intensity experience.
For the past 5 years, single-track mountain biking has been the all time single most enjoyable fitness activity in my life. Can't do a lot of the things I did years ago like heavy weight lifting and racquetball due to several injuries and subsequent shoulder surgeries. As I mentioned, as of late I have reduced weekly number of rides, riding intensity, and am taking more breaks. My hope is changing my diet to smaller multiple meals and the reduction in riding intensity will be enough. However, even if this were to work, I have no idea how long it would take that to trend in reduced episodes. No clue what the turn around of improvements is.
Not bragging but many times when I am on the trails and I see a guy near my age (which is rare) and if I do he is riding an E-assisted MTB. On those you can pedal the heavier bike as much as you want manually but can use the battery assistance anytime you feel you need it. I have always taken pride that I was still climbing these hills manually at my age. But in thinking about it recently maybe they are simply MUCH smarter than me. They are not cheap bikes but light years cheaper than a stroke or MI. If that is the route I have to go to continue to ride AND reduce the risk of Afib then I am ready pursue that route.
Up until the past couple of months I simply refused to believe it could be the amount of biking I was doing. That was a combination of my ignorance of the Afib topic and the fact that my endurance had actually increased AND the fact that these episodes have NEVER occurred the night of a mountain bike ride earlier in the day. Turns out any of the contributing factors can have a cumulative and delayed onset which make its more difficult to try to self diagnose.
Anyway, thank you for your info.
|
Re: New to Afib and requesting high Potassium advice October 03, 2021 08:45PM |
Registered: 5 years ago Posts: 108 |
My recommendation would be to get your RBC Mg tested at request a test. Dr. Denis Goodman in his book Magnificent Magnesium says that below 5.5 mg/dl is flirting with an arrhythmia. Everyone here likes the EXAtest better, which checks all of the minerals, so you may want your doc to order one of those.
Great idea to extend your eating window a little bit and end it earlier. Dr. Day's book The Afib Cure says that stuffing yourself can be a trigger.
I would also recommend stopping more often while Mtn biking, take some deep breaths, pull out your phone and take a few photos!! Slow down
Try yoga when you aren't biking or lifting. the ap "fit on" has some great short videos for men.
You and George N. sound like two peas in a pod!
Great idea to extend your eating window a little bit and end it earlier. Dr. Day's book The Afib Cure says that stuffing yourself can be a trigger.
I would also recommend stopping more often while Mtn biking, take some deep breaths, pull out your phone and take a few photos!! Slow down
Try yoga when you aren't biking or lifting. the ap "fit on" has some great short videos for men.
You and George N. sound like two peas in a pod!
|
Re: New to Afib and requesting high Potassium advice October 04, 2021 12:36PM |
Registered: 12 years ago Posts: 4,534 |
Quote
MarkL
Up until the past couple of months I simply refused to believe it could be the amount of biking I was doing. That was a combination of my ignorance of the Afib topic and the fact that my endurance had actually increased AND the fact that these episodes have NEVER occurred the night of a mountain bike ride earlier in the day. Turns out any of the contributing factors can have a cumulative and delayed onset which make its more difficult to try to self diagnose.
What I observed is the more intense and longer duration the activity, the more delayed the onset of my afib. As mentioned, my first afib episode was several days after a training run on a 14,000' peak. I was training for a race I'd done many times before, the Pikes Peak Ascent, which tops out over 14,000' and gains about 7,800' over 13 1/3 miles. I didn't understand initially that I should not do that race, actually I continued to do the race for a couple of years. My first episode was in early July 2004, the race is around the 3rd week in August, so I did it that year. A week or two after the race, I had an episode that didn't convert for 2 1/2 months. The race may have been the precipitating factor for the non-converting episode (which was ultimately converted with a loading dose of flecainide. I ran the race two years later, I don't recall if I had an episode after, but I do remember that my resting heart rate stayed much higher than usual for several days after the raced, an indication of the stress I was incurring. Then the resting rate would drop below my normal rate and I recall this being an afib risk period. Then the rate finally came back to normal.
I don't think the average cardio or even EP appreciates the contribution of aggressive exercise to afib. Percentage wise, most afibbers are sedentary, so this is the population most will see. For these folks, the data suggest that adding moderate exercise can improve their afib.
On fuel usage, I suggest the podcast with Iñigo San Millán I previously linked. Also, here are the detailed subscriber show notes (need to be loaded into a browser). From those notes is this graph:
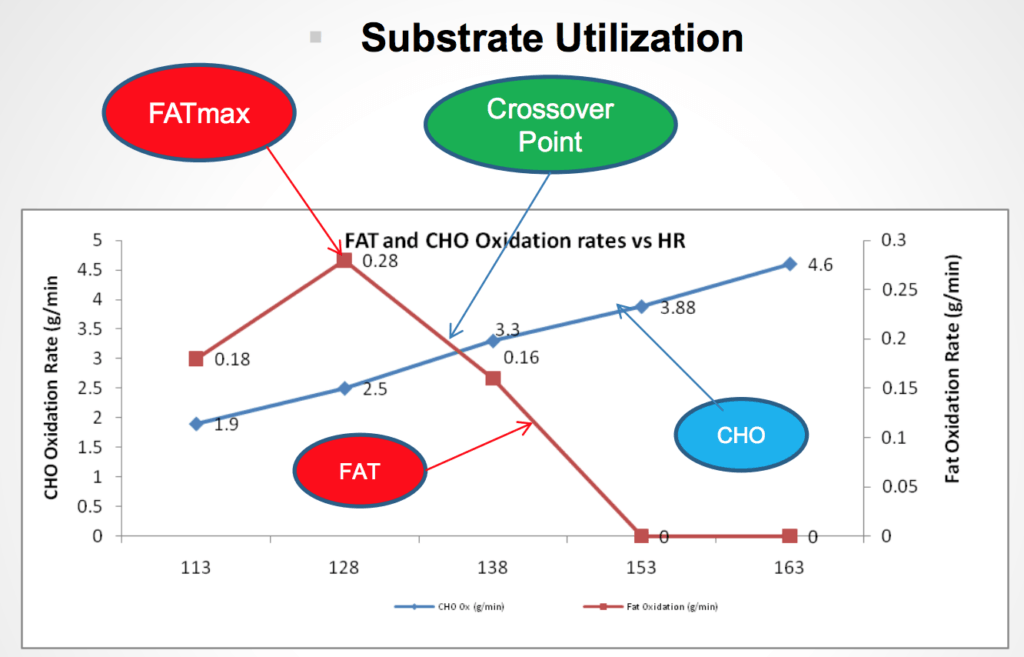
The heart rates on the bottom are just an example for one person, everybody's will be different, but the general curve shapes will be similar.
The idea is that at rest, we are using mostly fat for fuel along with some carbohydrate (CHO). The CHO use increases linearly with increased heart rate (exertion) and the fat utilization increases at a significantly faster rate till is drops very fast. Fat is the most efficient fuel, but as our energy needs increase, it can't make energy fast enough, so glucose takes over. At the FATMAX point and below, the metabolism is entirely aerobic, meaning there is enough oxygen to metabolize both the fat and the glucose through purely aerobic pathways. After that, anaerobic (without oxygen) pathways come into usage - gradually as effort increases. "A molecule of glucose can only produce three ATP molecules under anaerobic metabolism, while it produces 39 with aerobic metabolism." Source ATP is the cell's energy currency. Hence you can see the anaerobic pathways are much more inefficient. The cells make material amounts lactate, which is used as fuel, when the metabolism is anaerobic (clarifying, they always make lactate, but when going anaerobic, this materially increases). This lactate is processed by the slow twitch Type 1 muscle fibers. Lactate will accumulate in the serum (blood) above levels of 2.0 mmol/L. Very efficient athletes can produce huge amounts of energy without switching to anaerobic glucose production and they can also process very large amounts of lactate.
The takeaway is that the high end endurance athletes spent 80% of their training time in Zone 2 (which corresponds to FATMAX). This stimulates mitochondrial production and density in the Type 1 muscle fibers - up to a 4x increase in density. Most recreational athletes spend their time in higher zones, so they don't get this adaptation. I have a friend who has trained almost exclusively in Z2 for over 20 years. In physiology lab testing, his FATMAX heart rate is very close to his max heart rate. Meaning he can almost be going all out and still be in aerobic metabolism. In the graph the numbers by the points are the amount of fuel (fat or carbs grams/minute) metabolized per minute. Note that in the graph the FATMAX is 0.28 g/min. My friend tested at 1.9 grams of fat per minute! My friend calls his training "loafing." I posted about him here.
When I said my 10 minute high intensity sessions use the creatine phosphate energy system. This system uses stored ATP and only lasts a few seconds. It is anaerobic. However, I do avoid using the glucose anaerobic systems for any extended periods of time as I mentioned, my hypothesis is that this is the source of the excessive exercise trigger for afib. This purely my speculation and I have no data to support this statement.
Edited 1 time(s). Last edit at 10/04/2021 04:39PM by GeorgeN.
|
New to the group and new to afib October 04, 2021 03:46PM |
Registered: 3 years ago Posts: 1 |
I think I'm in shock and extreme fear after receiving confirmation of my diagnosis recently. I was convinced that anything.........anything.........related to the heart has to be a death sentence, for sure. I was shocked to hear the nurse tell
me that an ER trip is usually not necessary when afib hits. So, that gives you all a good idea for where I am with all this.......like
a sponge, reading all these resources that are available and hoping that with education, my panic and shock will soon subside.
Glad to have found this group..........Thank you!
me that an ER trip is usually not necessary when afib hits. So, that gives you all a good idea for where I am with all this.......like
a sponge, reading all these resources that are available and hoping that with education, my panic and shock will soon subside.
Glad to have found this group..........Thank you!
|
Re: New to the group and new to afib October 04, 2021 10:44PM |
Registered: 8 years ago Posts: 18,890 |
Hi MarkL and welcome -
Here’s a link to a past post on potassium…which includes the post: “Let’s Not Forget About Potassium”…
and you may find something helpful there.
[www.afibbers.org]
Jackie
PS - you can also go to Conference Room Session #31 and scan through the various posts that have
significant details about the relevancy of potassium levels, etc.
[www.afibbers.org]
Edited 1 time(s). Last edit at 10/04/2021 10:51PM by Jackie.
Here’s a link to a past post on potassium…which includes the post: “Let’s Not Forget About Potassium”…
and you may find something helpful there.
[www.afibbers.org]
Jackie
PS - you can also go to Conference Room Session #31 and scan through the various posts that have
significant details about the relevancy of potassium levels, etc.
[www.afibbers.org]
Edited 1 time(s). Last edit at 10/04/2021 10:51PM by Jackie.
|
***Update*** Re: New to Afib and requesting high Potassium advice December 05, 2021 10:00PM |
Registered: 3 years ago Posts: 15 |
Good afternoon, wanted to give an update on things since my original post in early October 2021. First, much thanks to everyone who responded both via this thread and via messages directly to me. Valuable information abounded.
In early October I took some advice I received here and did indeed switch meals from one large meal daily between 6:00pm-8:00pm to three smaller daily meals with the last being @ 6:00pm. I also restarted magnesium supplementation twice daily up to gut tolerance. Started cutting back on the number of mountain biking sessions per week and took longer breaks during those sessions, albeit not as much I should have.
Had my echocardiogram in October and it showed no issues (thank God) with valves, size or functioning. As a matter of fact, it showed an overall increase of 10% in my Ejection Fraction from two years ago, which was already in the normal range. I guess all the mountain biking did improve the plumbing but am thinking at the cost of some electrical circuitry. Since I changed the diet and reduced training, I have only had 2 episodes in the past two months. At my annual Cardiology appointment in mid-November, she was encouraged by the improvement but, since I have no real symptoms during episodes, wanted me to wear another ZioPatch round to see if anything was happening that I wasn’t detecting with my own physical feeling, especially during the night while asleep. She has also scheduled me with an EP to review the results of all of this in early January. I am currently at the end of week 1 of wearing the ZioPatch. I know of no issues so far, but we’ll see when the report comes back from iRythm.
So, I went from 3 to 4 episodes per month (and sometimes 2 weekly) to now 2 in two months. Not naïve enough to celebrate because I have NO doubt it will recur. However, maybe I am heading in the right direction. Simply to note, the 2 most recent episodes were, in both cases, I think because I started feeling ballsy again and slipped back into too many MTB sessions. Am backing ALL training back to Zone 2 or less with less frequency indefinitely going forward. I really enjoy training hard, but this stuff is way too scary to taunt. MUCH thanks to George for all the input on over-training. I KNOW that has been a major factor for me.
One interesting (to me anyway) sidenote is that these last 2 episodes were resolved in under 90 minutes by the following protocol: Once I noticed the episodes, I chewed 0.1mg Catapres, 81mg aspirin, and 0.5mg Xanax. Resolving in less than 90 minutes is new for me. I had read about the aspirin and Xanax in two separate other posts on this forum back in October and made a note of them. The Catapres was prescribed for me @ 7 years ago when I was switching from Lisinopril to Telmisartan for better BP control. Doctor told me to monitor my BP for a week when I switched and to take a Catapres if my BP went over 140/90 and stayed there or my HR went over 90 and stayed there. Anyway, that’s where the idea came from. I never needed to take it during the med switch but I kept the bottle of tabs all these years just in case. Maybe just a coincidence but I’ll certainly try it again when a future episode occurs.
I hope everyone has a wonderful Christmas season and a very NSR New Year.
In early October I took some advice I received here and did indeed switch meals from one large meal daily between 6:00pm-8:00pm to three smaller daily meals with the last being @ 6:00pm. I also restarted magnesium supplementation twice daily up to gut tolerance. Started cutting back on the number of mountain biking sessions per week and took longer breaks during those sessions, albeit not as much I should have.
Had my echocardiogram in October and it showed no issues (thank God) with valves, size or functioning. As a matter of fact, it showed an overall increase of 10% in my Ejection Fraction from two years ago, which was already in the normal range. I guess all the mountain biking did improve the plumbing but am thinking at the cost of some electrical circuitry. Since I changed the diet and reduced training, I have only had 2 episodes in the past two months. At my annual Cardiology appointment in mid-November, she was encouraged by the improvement but, since I have no real symptoms during episodes, wanted me to wear another ZioPatch round to see if anything was happening that I wasn’t detecting with my own physical feeling, especially during the night while asleep. She has also scheduled me with an EP to review the results of all of this in early January. I am currently at the end of week 1 of wearing the ZioPatch. I know of no issues so far, but we’ll see when the report comes back from iRythm.
So, I went from 3 to 4 episodes per month (and sometimes 2 weekly) to now 2 in two months. Not naïve enough to celebrate because I have NO doubt it will recur. However, maybe I am heading in the right direction. Simply to note, the 2 most recent episodes were, in both cases, I think because I started feeling ballsy again and slipped back into too many MTB sessions. Am backing ALL training back to Zone 2 or less with less frequency indefinitely going forward. I really enjoy training hard, but this stuff is way too scary to taunt. MUCH thanks to George for all the input on over-training. I KNOW that has been a major factor for me.
One interesting (to me anyway) sidenote is that these last 2 episodes were resolved in under 90 minutes by the following protocol: Once I noticed the episodes, I chewed 0.1mg Catapres, 81mg aspirin, and 0.5mg Xanax. Resolving in less than 90 minutes is new for me. I had read about the aspirin and Xanax in two separate other posts on this forum back in October and made a note of them. The Catapres was prescribed for me @ 7 years ago when I was switching from Lisinopril to Telmisartan for better BP control. Doctor told me to monitor my BP for a week when I switched and to take a Catapres if my BP went over 140/90 and stayed there or my HR went over 90 and stayed there. Anyway, that’s where the idea came from. I never needed to take it during the med switch but I kept the bottle of tabs all these years just in case. Maybe just a coincidence but I’ll certainly try it again when a future episode occurs.
I hope everyone has a wonderful Christmas season and a very NSR New Year.
Sorry, only registered users may post in this forum.