Welcome to the Afibber’s Forum
Serving Afibbers worldwide since 1999
Moderated by Shannon and Carey
 |
 |
 |
 |
 |
 |
Home
>
AFIBBERS FORUM
>
Topic
Can’t figure out the triggers
Posted by beardman
|
Can’t figure out the triggers August 22, 2018 09:55PM |
Registered: 5 years ago Posts: 45 |
I was diagnosed with afib in March at random (more explanation in my previous thread). I have been taking a variety of supplements both via recommendations here, my own reading and my naturopaths suggestions. I am 36 years old and have zero interest in any pharmaceuticals.
I am in rhythm about 70% of the time in any given month, generally out of rhythm for 24-48 hours at a clip. I can count on martial arts putting me back into rhythm 9/10 times and a plateau program on the exercise bike will do it about half the time. I have been unable to figure out my trigger(s) though. Previously it was running so I switched to biking, now it seems to be completely at random. I record just about everything and it does not seem to relate to any specific time of day, physically activity, eating or drinking, lack of eating or drinking, temperature, stress level, I have even looked at clothing.
I check myself with my Kardia monitor and can generally tell 2-3 hours before I am going to kick out of rhythm. I start to feel crappy and feel a hollow feeling in my chest. During this time I show no abnormalities on my ecg until I kick out when my P wave disappears. I generally have a heart rate under 100bpm when out of rhythm and it is in the 50-60 range when in rhythm. When I sleep it is not unusual for it to drop down to 35-40. I tape my mouth shut when I sleep to force nasal breathing and have only once or twice kicked out of rhythm while sleeping. I did have a sleep study done, but it was inconclusive.
I am at my wits end, please help.
Joel
I am in rhythm about 70% of the time in any given month, generally out of rhythm for 24-48 hours at a clip. I can count on martial arts putting me back into rhythm 9/10 times and a plateau program on the exercise bike will do it about half the time. I have been unable to figure out my trigger(s) though. Previously it was running so I switched to biking, now it seems to be completely at random. I record just about everything and it does not seem to relate to any specific time of day, physically activity, eating or drinking, lack of eating or drinking, temperature, stress level, I have even looked at clothing.
I check myself with my Kardia monitor and can generally tell 2-3 hours before I am going to kick out of rhythm. I start to feel crappy and feel a hollow feeling in my chest. During this time I show no abnormalities on my ecg until I kick out when my P wave disappears. I generally have a heart rate under 100bpm when out of rhythm and it is in the 50-60 range when in rhythm. When I sleep it is not unusual for it to drop down to 35-40. I tape my mouth shut when I sleep to force nasal breathing and have only once or twice kicked out of rhythm while sleeping. I did have a sleep study done, but it was inconclusive.
I am at my wits end, please help.
Joel
|
Re: Can’t figure out the triggers August 22, 2018 10:32PM |
Registered: 8 years ago Posts: 1,102 |
Do you have an EP? That’s an electrophysiologist. Like a cardiologist but specializing in the heart’s electrical system. I’m sorry if I’m repeating myself because I think you’ve posted before, but an EP is definitely where you want to go. It sounds like vagally-mediated AF due to chronic fitness (something I know something about). That generally makes one an excellent ablation candidate, barring any other serious comorbidities.
Triggers can be obvious for some and complete mysteries for others. Don’t lose heart (pun intended) if you’re in the latter category. Once an experienced EP gets in there with his or her mapping catheter then the mystery can be solved.
Triggers can be obvious for some and complete mysteries for others. Don’t lose heart (pun intended) if you’re in the latter category. Once an experienced EP gets in there with his or her mapping catheter then the mystery can be solved.
|
Re: Can’t figure out the triggers August 22, 2018 11:42PM |
Registered: 5 years ago Posts: 45 |
I do and I am sure this is just me being stubborn, but I really didn’t like the path he wanted me to go down. He was insistent on an electro cardioversion and wanted me on blood thinners and a few other things to, “try them out”. My chads vast number is zero. I suggested that I could wait a few days to kick back into NSR and it was like I had just insulted him. I have read so many mixed reviews on the ablations and I just don’t think I’m ready for that step yet.
My echo is perfect and stress tests show no blockages. I know the risks, but I just feel with being younger that I don’t want to be making a choice that doesn’t have to be done immediately. I figure a wrong choice now could impact the next 40 years . . .
I have tried accupunture and chiropractic to target the Vagus Nerve. I have also tried all the tricks like cold water, bearing down, cold showers. Nothing seems to make an impact.
My echo is perfect and stress tests show no blockages. I know the risks, but I just feel with being younger that I don’t want to be making a choice that doesn’t have to be done immediately. I figure a wrong choice now could impact the next 40 years . . .
I have tried accupunture and chiropractic to target the Vagus Nerve. I have also tried all the tricks like cold water, bearing down, cold showers. Nothing seems to make an impact.
|
Re: Can’t figure out the triggers August 23, 2018 12:03AM |
Registered: 6 years ago Posts: 920 |
|
Re: Can’t figure out the triggers August 23, 2018 12:48AM |
Registered: 5 years ago Posts: 129 |
Quote
wolfpack
It sounds like vagally-mediated AF due to chronic fitness (something I know something about).
Curious I'm trying to get a handle on "vagally-mediated"
Is there a reason the chronically fit people would have vagally mediated afib? (reference?)
Was there something in his description of his symptoms that would indicate it is vagal? I guess I don't really how people tell vagal from non.
Which gets around to another question I've been having... there are all these things that seem to associate with afib... hypertension, obesity etc.
But of course association and causation are two different things.
I can see that that if longstanding hypertension has damaged (enlarged etc) your heart, that may be causative for afib. But say you are hypertensive and your heart is still normal, is it really the hypertension causing afib? Or is it merely associated, but not causative?
|
Re: Can’t figure out the triggers August 23, 2018 04:21AM |
Registered: 9 years ago Posts: 1,087 |
Did you ever follow up on an Endocrine/Cortisol check-up, as suggested in in your earlier Post? A Saliva Cortisol 4X/day test would tell what is going on with Adrenal output. The fact that you can sense it coming on several hours prior suggests some sort of intermittent Hormonal or Electrolytic imbalance. I had intermittent periods of Adrenal Suppression which triggered AFIB. I felt wiped out and unsually tired for about a day prior to my episodes.
|
Re: Can’t figure out the triggers August 23, 2018 06:26AM |
Registered: 7 years ago Posts: 218 |
Quote
The Anti-Fib
Did you ever follow up on an Endocrine/Cortisol check-up, as suggested in in your earlier Post? A Saliva Cortisol 4X/day test would tell what is going on with Adrenal output. The fact that you can sense it coming on several hours prior suggests some sort of intermittent Hormonal or Electrolytic imbalance. I had intermittent periods of Adrenal Suppression which triggered AFIB. I felt wiped out and unsually tired for about a day prior to my episodes.
What is the treatment/med or protocol you use for adrenal fatigue or high cortisol levels at night?
|
Re: Can’t figure out the triggers August 23, 2018 07:40AM |
Registered: 9 years ago Posts: 1,087 |
Quote
hwkmn05
Did you ever follow up on an Endocrine/Cortisol check-up, as suggested in in your earlier Post? A Saliva Cortisol 4X/day test would tell what is going on with Adrenal output. The fact that you can sense it coming on several hours prior suggests some sort of intermittent Hormonal or Electrolytic imbalance. I had intermittent periods of Adrenal Suppression which triggered AFIB. I felt wiped out and unsually tired for about a day prior to my episodes.
What is the treatment/med or protocol you use for adrenal fatigue or high cortisol levels at night?
I didn't have high levels at night, more on the low side. I was running out of Cortisol especially upon Stressful situations. I have a relatively rare condition of constant Thirst, and I was drinking way too many fluids, and was flushing out the Cortisol in my Urine. As for a treatment, I try to cut down on Water intake, even if I'm thirsty. Also I stopped taking Prednisone and getting Steriod injections for inflammation. I was intermittently taking the potent Drug Prednisone (boosts Cortisol) for Inflammation, and when I stopped taking it, my body did not make enough of its own Cortisol, and I had low Cortisol output for 7-10 days causing the "Adrenal Suppression" which triggered my AFIB. Now if i feel wiped out, I take a low dose of Hydrocortisone (Stress Dosing) to temporarily boost up my Cortisol levels. I have been doing well since I made this change. Almost 10 years into AFIB, never been doing better. No Ablation or Anti-Arrythmics.
Edited 1 time(s). Last edit at 08/23/2018 07:58AM by The Anti-Fib.
|
Re: Can’t figure out the triggers August 23, 2018 08:40AM |
Registered: 5 years ago Posts: 45 |
Quote
Pompon
Your doc is right when he wants having you back in NSR as soon as possible. Waiting is usually bad because the longer you're in afib, the more likely afib would worsen.
I understand this, but with the ability to convert on my own, I just didn't feel it was necessary. I am usually in NSR for 3-4 days at a clip and then out for 1-2 days.
|
Re: Can’t figure out the triggers August 23, 2018 08:51AM |
Registered: 5 years ago Posts: 45 |
Quote
The Anti-Fib
Did you ever follow up on an Endocrine/Cortisol check-up, as suggested in in your earlier Post? A Saliva Cortisol 4X/day test would tell what is going on with Adrenal output. The fact that you can sense it coming on several hours prior suggests some sort of intermittent Hormonal or Electrolytic imbalance. I had intermittent periods of Adrenal Suppression which triggered AFIB. I felt wiped out and unsually tired for about a day prior to my episodes.
I did and thought I had posted the results (which are not right at my fingertips right now). My cortisol levels where fine, but my DHEA numbers where through the roof. The numbers all followed the curve of the chart, but I want to say that my DHEA numbers where in the range of 900-1,200 area. My doctor prescribed me Adrenotone from Designs by Health to counteract this. Adrenotone I am scheduled to take another test within the next month to see how/if this has helped.
The other supplements that I am taking are:
1 grams L-Argentine 3X daily
1 gram Vitamin C 3X daily
500mg Niavasc (Niacin) 1X daily
20,000 fu Nattokinase 1X daily
3 caps Adrenotone 3X daily
200mg DHA form Algae 3X daily
1 cap Vitamin D Supreme (5,000iu Vit D and 550mcg Vit K) 1X daily
I generally don't feel tired leading up to an episode, it is only when I am on the tailend of an episode that I get wiped out (after being out of rhythm for 24-48hrs).
Edited 1 time(s). Last edit at 08/23/2018 08:53AM by beardman.
|
Re: Can’t figure out the triggers August 23, 2018 10:06AM |
Registered: 8 years ago Posts: 1,102 |
Beardman,
Your EP is really just following standard procedure for paroxysmal AF patients. It's cardioversion within 48 hours of onset, followed by anticoagulation and AAR/rate control meds. He isn't using you as a "guinea pig" by any means. I can certainly understand not wanting to do that on your part, but do bear in mind that you really want to minimize the time in AF or else it will just get worse. 2 days on, 3 days off is actually a fairly high burden. I know you've said the rate isn't terribly high during an episode, but it will still "wear" on the ventricles after some time.
Your EP is really just following standard procedure for paroxysmal AF patients. It's cardioversion within 48 hours of onset, followed by anticoagulation and AAR/rate control meds. He isn't using you as a "guinea pig" by any means. I can certainly understand not wanting to do that on your part, but do bear in mind that you really want to minimize the time in AF or else it will just get worse. 2 days on, 3 days off is actually a fairly high burden. I know you've said the rate isn't terribly high during an episode, but it will still "wear" on the ventricles after some time.
|
Re: Can’t figure out the triggers August 23, 2018 10:19AM |
Registered: 8 years ago Posts: 1,102 |
Quote
bolimasa
Curious I'm trying to get a handle on "vagally-mediated"
Is there a reason the chronically fit people would have vagally mediated afib? (reference?)
Was there something in his description of his symptoms that would indicate it is vagal? I guess I don't really how people tell vagal from non.
Which gets around to another question I've been having... there are all these things that seem to associate with afib... hypertension, obesity etc.
But of course association and causation are two different things.
I can see that that if longstanding hypertension has damaged (enlarged etc) your heart, that may be causative for afib. But say you are hypertensive and your heart is still normal, is it really the hypertension causing afib? Or is it merely associated, but not causative?
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1767580/
Vagally-mediated AF is characterized by episodes beginning at rest, often nighttimes, or post-prandially. It is likely an imbalance in autonomic nervous system within the atria in which the parasympathetic (vagal) nerves overwhelm the sympathetic nerves. It is a common side-effect of exercise (AF is something like 5x more prevalent in the athletic community versus the general population).
Think of it like this - when you condition the heart to pump blood very efficiently, my guess is that it needs to retain the ability to "go slow" more than it needs the ability to "go fast" because everyone spends more time at rest than they do at activity. Even if a runner, swimmer, or cyclist spends 1 or 2 hours a day with an elevated pulse due to activity, that still leaves 22-23 hours a day where the heart output needs to meet the lower oxygen demands of being at rest. So to keep the blood pressure low enough, the body will create more parasympathetic tone in the heart to signal the atrial cells to be more refractory (slow down).
In a nutshell, if you're going into AF when you're exerting yourself, you're not vagal. You're adrenergic, or possibly mixed.
|
Re: Can’t figure out the triggers August 23, 2018 10:31AM |
Registered: 7 years ago Posts: 218 |
Quote
wolfpack
Beardman,
Your EP is really just following standard procedure for paroxysmal AF patients. It's cardioversion within 48 hours of onset, followed by anticoagulation and AAR/rate control meds. He isn't using you as a "guinea pig" by any means. I can certainly understand not wanting to do that on your part, but do bear in mind that you really want to minimize the time in AF or else it will just get worse. 2 days on, 3 days off is actually a fairly high burden. I know you've said the rate isn't terribly high during an episode, but it will still "wear" on the ventricles after some time.
I learned the hard way about converting, electrically or chemically. Im in the camp of, ASAP the better. My rate was usually low and quite irregular, but nonetheless, sleep was nearly impossible. You only open yourself up to the need for more meds and precautions by waiting.
|
Re: Can’t figure out the triggers August 23, 2018 10:45AM |
Registered: 7 years ago Posts: 218 |
Quote
The Anti-Fib
Did you ever follow up on an Endocrine/Cortisol check-up, as suggested in in your earlier Post? A Saliva Cortisol 4X/day test would tell what is going on with Adrenal output. The fact that you can sense it coming on several hours prior suggests some sort of intermittent Hormonal or Electrolytic imbalance. I had intermittent periods of Adrenal Suppression which triggered AFIB. I felt wiped out and unsually tired for about a day prior to my episodes.
What is the treatment/med or protocol you use for adrenal fatigue or high cortisol levels at night?
I didn't have high levels at night, more on the low side. I was running out of Cortisol especially upon Stressful situations. I have a relatively rare condition of constant Thirst, and I was drinking way too many fluids, and was flushing out the Cortisol in my Urine. As for a treatment, I try to cut down on Water intake, even if I'm thirsty. Also I stopped taking Prednisone and getting Steriod injections for inflammation. I was intermittently taking the potent Drug Prednisone (boosts Cortisol) for Inflammation, and when I stopped taking it, my body did not make enough of its own Cortisol, and I had low Cortisol output for 7-10 days causing the "Adrenal Suppression" which triggered my AFIB. Now if i feel wiped out, I take a low dose of Hydrocortisone (Stress Dosing) to temporarily boost up my Cortisol levels. I have been doing well since I made this change. Almost 10 years into AFIB, never been doing better. No Ablation or Anti-Arrythmics.
Interesting. After my 6 time interval saliva test, I was low daytime and high in the evening. DHEA and HPA Adapt cortisol manager daytime and Seriphos, HPA Stress Hormone stabilizer at night. No episodes for 16 months since. We shall see if this was it after 8 years.
|
Re: Can’t figure out the triggers August 23, 2018 10:54AM |
Registered: 6 years ago Posts: 18,881 |
Joel/Beardman - The Adrenotone may be too stimulating... esp. in combo with L-arginine. The Adrenotone product data sheet has this notation:
Advise patient to discontinue use and consult you if they experience sleeplessness, headache or
heart palpitations when using Adrenotone™.
You should consider cutting back on the arginine as well as that can be too stimulatory for some individuals .... (or just stop completely for a while).
Also - what's your source of magnesium ? Most people can't get enough from food and supplements are needed. Have you assessed your daily intake of potassium from food sources? Those who do endurance athletics and also are plagued by arrhythmia and/or ectopy need to be sure they have the right balance of electrolytes that affect heart cell function.
Jackie
Advise patient to discontinue use and consult you if they experience sleeplessness, headache or
heart palpitations when using Adrenotone™.
You should consider cutting back on the arginine as well as that can be too stimulatory for some individuals .... (or just stop completely for a while).
Also - what's your source of magnesium ? Most people can't get enough from food and supplements are needed. Have you assessed your daily intake of potassium from food sources? Those who do endurance athletics and also are plagued by arrhythmia and/or ectopy need to be sure they have the right balance of electrolytes that affect heart cell function.
Jackie
|
Re: Can’t figure out the triggers August 23, 2018 12:31PM |
Registered: 5 years ago Posts: 45 |
Quote
Jackie
Joel/Beardman - The Adrenotone may be too stimulating... esp. in combo with L-arginine. The Adrenotone product data sheet has this notation:
Advise patient to discontinue use and consult you if they experience sleeplessness, headache or
heart palpitations when using Adrenotone™.
You should consider cutting back on the arginine as well as that can be too stimulatory for some individuals .... (or just stop completely for a while).
Also - what's your source of magnesium ? Most people can't get enough from food and supplements are needed. Have you assessed your daily intake of potassium from food sources? Those who do endurance athletics and also are plagued by arrhythmia and/or ectopy need to be sure they have the right balance of electrolytes that affect heart cell function.
Jackie
I will speak to my doctor about the Adrenotone today and try dropping the L-Arginine for a while as well.
For Magnesium I was taking THIS for a while, but showed zero difference in the amount of time I was in NSR. Ultimately I would prefer to be on as few supplements as possible, as I am sure would everyone.
I also tried taking Potassium Gluconate Power for about a month. I am figuring that I consume under 1000MG a day so I was taking 2.5 tablespoons/day spread out to try to hit ~3,500 total MG/day. Again, no difference so I discontinued usage.
|
Re: Can’t figure out the triggers August 23, 2018 04:13PM |
Registered: 11 years ago Posts: 4,226 |
Quote
beardman
Your doc is right when he wants having you back in NSR as soon as possible. Waiting is usually bad because the longer you're in afib, the more likely afib would worsen.
I understand this, but with the ability to convert on my own, I just didn't feel it was necessary. I am usually in NSR for 3-4 days at a clip and then out for 1-2 days.
I would say that an electro cardioversion would be pointless, it would shorten that event but won't likely prevent the next one. You need a plan to stay in rhythm after you convert.
You don't want meds, but perhaps flecainide on demand might do a quick conversion. Not a forever solution, but at least would minimize the AF burden while you try to figure out triggers.
Even though exercise will convert you, it is also likely part of the problem. It certainly was for me <[www.afibbers.org]
George
|
Re: Can’t figure out the triggers August 23, 2018 04:25PM |
Registered: 9 years ago Posts: 1,087 |
Quote
wolfpack
Beardman,
Your EP is really just following standard procedure for paroxysmal AF patients. It's cardioversion within 48 hours of onset, followed by anticoagulation and AAR/rate control meds. He isn't using you as a "guinea pig" by any means. I can certainly understand not wanting to do that on your part, but do bear in mind that you really want to minimize the time in AF or else it will just get worse. 2 days on, 3 days off is actually a fairly high burden. I know you've said the rate isn't terribly high during an episode, but it will still "wear" on the ventricles after some time.
I disagree, the EP was making an quick remark off the top of his head, and not thinking through the situation completely.
ECV would be warranted if there was an indefinate time until self-conversion, not a window of 1-3 days. Beardman cannot get an ECV every Week. All of the Dr's and Nurses at the Hospital would not want to be part of that, and neither should the patient. It would be hard to imagine any EP ordering over maybe 12 EVC's for a patient a year. At some point the EP, and others involved would stop cooperating, and demand other means like Ablation.
|
Re: Can’t figure out the triggers August 23, 2018 04:30PM |
Registered: 11 years ago Posts: 4,226 |
Quote
bolimasa
It sounds like vagally-mediated AF due to chronic fitness (something I know something about).
Curious I'm trying to get a handle on "vagally-mediated"
Is there a reason the chronically fit people would have vagally mediated afib? (reference?)
Was there something in his description of his symptoms that would indicate it is vagal? I guess I don't really how people tell vagal from non.
Fit folks get it because they have high vagal tone. The high vagal tone is why Lance Armstrong had a resting heart rate in the low 30's, at least at one point. Most of us who are chronically fit have resting heart rates in the 50's or lower. In my experience it is a change (dynamic increase) in vagal tone on top of an already high vagal tone that is the trigger. For example, I over exercise, then have dinner and am relaxing after dinner (all increasing vagal tone). Then an episode occurs.
The fact that beardman can convert some episodes with exercise is a vagal characteristic. Typically a vagal won't go into an episode during exercise, while an adrenergic person will. Of course there are those with "mixed" triggers, in which case all bets are off (which you could be).
Quote
bolimasa
Which gets around to another question I've been having... there are all these things that seem to associate with afib... hypertension, obesity etc.
But of course association and causation are two different things.
I can see that that if longstanding hypertension has damaged (enlarged etc) your heart, that may be causative for afib. But say you are hypertensive and your heart is still normal, is it really the hypertension causing afib? Or is it merely associated, but not causative?
As far as I'm aware, it is association, though a fairly strong one. It is the reason why some of those with these issues can have their afib get better when they get rid of these issues.
I know that on a larger heart, it is easier for the reentrant afib wavelets to propagate. Hence tall people are also at higher risk. I know there are discussions on this in the archives from 12 or so years ago.
Surgery in the heart area, even lung, can cause afib. I believe this is because of the inflammation caused by the surgery. Perhaps the hypertension causes some inflammation?????
George
|
Re: Can’t figure out the triggers August 23, 2018 04:34PM |
Registered: 5 years ago Posts: 45 |
Quote
GeorgeN
Your doc is right when he wants having you back in NSR as soon as possible. Waiting is usually bad because the longer you're in afib, the more likely afib would worsen.
I understand this, but with the ability to convert on my own, I just didn't feel it was necessary. I am usually in NSR for 3-4 days at a clip and then out for 1-2 days.
I would say that an electro cardioversion would be pointless, it would shorten that event but won't likely prevent the next one. You need a plan to stay in rhythm after you convert.
You don't want meds, but perhaps flecainide on demand might do a quick conversion. Not a forever solution, but at least would minimize the AF burden while you try to figure out triggers.
Even though exercise will convert you, it is also likely part of the problem. It certainly was for me <[www.afibbers.org]
George
I completely agree with your option about the electro cardioversion which is why I didn’t do it. My EP suggested that I take flecainide, but cautioned me that I absolutely couldn’t take it before the cardioversion as it could put me into NSR which could throw a clot. I know they are going by the book and I don’t want a stroke, but I just wish I could find the balance a little better.
I consume 1,000-1,500 MG of calcium a day, maybe that’s too much and I could try cutting down. I eat a Keto/vegetarian diet though, so I am sourcing most of my fat content from dairy.
I certainly am not doing endurance training and I have cut my exercise down to 5-10 hours per week. I don’t for a second doubt that there is a chemical/electrolyte imbalance. Some days doing the exact same workout in an attempt to convert just won’t work. There must be another variable.
|
Re: Can’t figure out the triggers August 23, 2018 04:41PM |
Registered: 11 years ago Posts: 4,226 |
Quote
beardman
I consume 1,000-1,500 MG of calcium a day, maybe that’s too much and I could try cutting down. I eat a Keto/vegetarian diet though, so I am sourcing most of my fat content from dairy.
From my experience, I'd stop the Ca++ completely. Now. When I was overeating Ca++ , I had many more triggers. I'm much more robust without it.
How much is too much exercise is too much is likely very individual.
In your shoes, I'd cut the Ca++ and also go to no material exercise and see what happens. If all is good, then I'd gradually add in exercise and see what level is triggering. I'm an "endpoint" guy. I like to start from known "good" and then work from there. Hence I'ld try ditching the Ca and the exercise and see what happens. If it is all good, then you can add back. If that doesn't do it, then you have to think what your next step is.
George
|
Re: Can’t figure out the triggers August 23, 2018 04:53PM |
Registered: 5 years ago Posts: 45 |
Quote
GeorgeN
I consume 1,000-1,500 MG of calcium a day, maybe that’s too much and I could try cutting down. I eat a Keto/vegetarian diet though, so I am sourcing most of my fat content from dairy.
From my experience, I'd stop the Ca++ completely. Now. When I was overeating Ca++ , I had many more triggers. I'm much more robust without it.
How much is too much exercise is too much is likely very individual.
In your shoes, I'd cut the Ca++ and also go to no material exercise and see what happens. If all is good, then I'd gradually add in exercise and see what level is triggering. I'm an "endpoint" guy. I like to start from known "good" and then work from there. Hence I'ld try ditching the Ca and the exercise and see what happens. If it is all good, then you can add back. If that doesn't do it, then you have to think what your next step is.
George
I appreciate the input. I did stop any workouts other than martial arts for about a month and that didn’t have any effect.
I then stopped all training/exercise for a week a couple of weeks ago and spent 8 full days out of NSR. I won’t be doing that again. I’ll try dropping my cheese/dairy intake and see what that does for a week or so.
Edited 1 time(s). Last edit at 08/23/2018 04:54PM by beardman.
|
Re: Can’t figure out the triggers August 23, 2018 06:50PM |
Registered: 11 years ago Posts: 4,226 |
Quote
beardman
I’ll try dropping my cheese/dairy intake and see what that does for a week or so.
I think mine is about 500-600mg/day. It was stress eating wheels of brie during my divorce that was the culprit for me. I had a before and after. I started this stress habit fairly soon after the divorce ensued. I was eating a keto diet at the time (now it is ovo-pescatarian vegan keto), so thought I had a "free pass." I thought stress was the reason my triggers got MUCH more sensitive. I thought I had a lot more remodeling and that was just too bad and a trip to Dr. N in Austin was my next option. Took me 18 months to go back to the literature and realize that it could be Ca++. I quit the cheese and my control went back to pre divorce stress levels.
|
Re: Can’t figure out the triggers August 24, 2018 05:49AM |
Registered: 5 years ago Posts: 45 |
Has anyone noticed or been measuring their heart rate variability? Mine is measure automatically with my Apple Watch. When in NSR it is between 20-75, but when out of rhythm it spikes upwards of 250ms. I am not sure if the watch is accurate during an arrhythmia or if this is another valuable piece of data to follow.
Without changing anything yet, I worked out at martial arts for about a hour last night with varying degrees of exertion and went back into NSR. I then went and did a slow paced bike for about 6 miles/20 minutes at the gym, still all good. We’ll see how long this lasts . . .
Without changing anything yet, I worked out at martial arts for about a hour last night with varying degrees of exertion and went back into NSR. I then went and did a slow paced bike for about 6 miles/20 minutes at the gym, still all good. We’ll see how long this lasts . . .
|
Re: Can’t figure out the triggers August 24, 2018 09:45AM |
Registered: 6 years ago Posts: 18,881 |
Beardman - your intake of calcium... I consume 1,000-1,500 MG of calcium a day is very high.
You need to cut back to under 500 mg or less... on a permanent basis. ... because calcium is excitatory to cells... that includes heart cells. And it will dominate over magnesium... (which is calming or relaxing)..... If your magnesium intake is consistently low, then that explains the problems you are experiencing. Most afibbers need to supplement with magnesium continually... especially those who are heavy exercisers.... and it needs to be the form of magnesium that reaches the interior of the cell without interference.
There is a book written by a cardiologist... Thomas E. Levy, MD, JD... titled Death by Calcium.... and he goes into all the details as to why calcium intake is so detrimental to the body on many levels. We need some calcium but not nearly the amount that many people take in daily.
Jackie
You need to cut back to under 500 mg or less... on a permanent basis. ... because calcium is excitatory to cells... that includes heart cells. And it will dominate over magnesium... (which is calming or relaxing)..... If your magnesium intake is consistently low, then that explains the problems you are experiencing. Most afibbers need to supplement with magnesium continually... especially those who are heavy exercisers.... and it needs to be the form of magnesium that reaches the interior of the cell without interference.
There is a book written by a cardiologist... Thomas E. Levy, MD, JD... titled Death by Calcium.... and he goes into all the details as to why calcium intake is so detrimental to the body on many levels. We need some calcium but not nearly the amount that many people take in daily.
Jackie
|
Re: Can’t figure out the triggers August 24, 2018 10:56AM |
Registered: 6 years ago Posts: 444 |
Quote
Jackie
Beardman - your intake of calcium... I consume 1,000-1,500 MG of calcium a day is very high.
You need to cut back to under 500 mg or less... on a permanent basis.
Jackie, I think everyone is different and needs to do their own research. Calcium is an important nutrient and quotes closer to 1200 mg, especially for people over age 50 are prevalent. There are lots of studies and uncertainties, and I don't believe anyone is qualified to be making statements about what people need to be doing on this board.
Edited 1 time(s). Last edit at 08/24/2018 10:57AM by jpeters.
|
Re: Can’t figure out the triggers August 24, 2018 11:22AM |
Registered: 8 years ago Posts: 1,102 |
A healthy, adult male between the ages of 18 and 60 could probably exist just fine on 0mg of dietary calcium per day. You really don't need it. In terms of electrolyte gradients across cardiac cells, Ca2+ concentration is something like 4 orders of magnitude less on the inside vs outside.
Edited 1 time(s). Last edit at 08/24/2018 03:00PM by wolfpack.
Edited 1 time(s). Last edit at 08/24/2018 03:00PM by wolfpack.
|
Re: Can’t figure out the triggers August 24, 2018 11:36AM |
Registered: 5 years ago Posts: 129 |
Quote
wolfpack
Curious I'm trying to get a handle on "vagally-mediated"
Is there a reason the chronically fit people would have vagally mediated afib? (reference?)
Was there something in his description of his symptoms that would indicate it is vagal? I guess I don't really how people tell vagal from non.
Which gets around to another question I've been having... there are all these things that seem to associate with afib... hypertension, obesity etc.
But of course association and causation are two different things.
I can see that that if longstanding hypertension has damaged (enlarged etc) your heart, that may be causative for afib. But say you are hypertensive and your heart is still normal, is it really the hypertension causing afib? Or is it merely associated, but not causative?
[www.ncbi.nlm.nih.gov]
Vagally-mediated AF is characterized by episodes beginning at rest, often nighttimes, or post-prandially. It is likely an imbalance in autonomic nervous system within the atria in which the parasympathetic (vagal) nerves overwhelm the sympathetic nerves. It is a common side-effect of exercise (AF is something like 5x more prevalent in the athletic community versus the general population).
Think of it like this - when you condition the heart to pump blood very efficiently, my guess is that it needs to retain the ability to "go slow" more than it needs the ability to "go fast" because everyone spends more time at rest than they do at activity. Even if a runner, swimmer, or cyclist spends 1 or 2 hours a day with an elevated pulse due to activity, that still leaves 22-23 hours a day where the heart output needs to meet the lower oxygen demands of being at rest. So to keep the blood pressure low enough, the body will create more parasympathetic tone in the heart to signal the atrial cells to be more refractory (slow down).
In a nutshell, if you're going into AF when you're exerting yourself, you're not vagal. You're adrenergic, or possibly mixed.
Thanks for the info.
And thanks for the new to me word - "prandially" I'd never heard that one before, and always enjoy an opportunity to learn a new word.
Your description makes me wonder if I am 'mixed'.
Certainly my medical test indicated Afib under exertion, Kinda makes me wonder if this relates to me being a "bad uphill girl" something I've struggled with my whole life. Has my heart always gone a little wacky when I hit that certain exertion point? I wish there was a way to know.
It would be easier to figure all this out if I could really tell when I am in afib... I also wonder about the vagal issue. One odd thing I've been trying to figure out is if there is a link between my pulsitile tinnitus and my afib... I started getting the pulsitile tinnitus ~ 2 years prior to my afib diagnosis. I don't have it all the time, or at least don't notice it all the time, but when I do hear it is when I rest on my couch in the evening and when I go to bed. Now I'm wondering if I am more afibby at this time. I have also noticed that of the few times I could really tell I am in afib, those events happened at night in bed.
Maybe none of this **really** matters... but maybe it would be good for me to understand my patterns (if they exist) so I can best assess my ablation recovery.
|
Re: Can’t figure out the triggers August 24, 2018 11:40AM |
Registered: 6 years ago Posts: 444 |
|
Re: Can’t figure out the triggers August 24, 2018 12:55PM |
Registered: 6 years ago Posts: 18,881 |
jpeters - There is plenty of reliable documentation to support the problem with excess calcium - especially in afibbers and we've been pointing to the reasons why since the forum first began.
In the book, Death by Calcium, by cardiologist Thomas E. Levy, MD, JD... there are several topic titles that refute the calcium need. A sample of the topic titles and 'headlines'
Chapt. 1 Is Calcium Really a Killer?
Impartial Science Delivers a "Guilty" Verdict
Excess Calcium Promotes Heart Disease
You are 30% more likely to have a heart attack and up to 20% more likely to have a stroke if you take an an extra 500 mg of calcium or more per day- that's the consensus derived from a comprehensive review of 15 independent clinical investigations. The reviewing researchers reported that subjects taking calcium supplements (500 mg or more per day) had 27 to 31% high risk of heart attack and 12 to 20% greater risk of stroke.
Dump more calcium into the caldron and the brew becomes even more deadly. A study of over 61,000 participants viewed over a 19-year period concludes that those with calcium intakes over 1400 mg/day had an alarming 40% increased risk of death from cardiovascular disease in general and a 114% increase in risk of death from reduced flow of blood to the heart muscle (ischemic heart disease.)... . these are footnote references
Also...other segment topics ...
Excess Calcium Promotes Cancer....
Excess Calcium & Toxins promote Increased Cellular Dysfunction and Death
Excess Calcium Increases Death Rate from All Diseases
The Toxicity of Calcium Supplementation
Calcium's Deadly Myths
Untangling Fact from Fiction
Myth #1 "Calcium supplementation and increased dietary calcium are good for you"
Myth #2 "You cannot get enough calcium in your diet without dairy products."
Myth #3 "Everyone with osteoporosis has a calcium deficiency"
(3 out of 8 elaborations)
Dr. Levy is not alone in presenting the risks of excess calcium in the body. Fortunately, there are many medical professionals giving similar advice and precautions based on the science. The problem is basically, that it's easy to get a lot of calcium from common dietary intake. Not so easy to get optimal magnesium... which has been a common focus here and should remain so as it definitely has an influence on excitability of cardiac cells and that's basic science.
Jackie
Death by Calcium
Thomas E. Levy, MD, JD
MedFox Publishing
Copyright 2013
In the book, Death by Calcium, by cardiologist Thomas E. Levy, MD, JD... there are several topic titles that refute the calcium need. A sample of the topic titles and 'headlines'
Chapt. 1 Is Calcium Really a Killer?
Impartial Science Delivers a "Guilty" Verdict
Excess Calcium Promotes Heart Disease
You are 30% more likely to have a heart attack and up to 20% more likely to have a stroke if you take an an extra 500 mg of calcium or more per day- that's the consensus derived from a comprehensive review of 15 independent clinical investigations. The reviewing researchers reported that subjects taking calcium supplements (500 mg or more per day) had 27 to 31% high risk of heart attack and 12 to 20% greater risk of stroke.
Dump more calcium into the caldron and the brew becomes even more deadly. A study of over 61,000 participants viewed over a 19-year period concludes that those with calcium intakes over 1400 mg/day had an alarming 40% increased risk of death from cardiovascular disease in general and a 114% increase in risk of death from reduced flow of blood to the heart muscle (ischemic heart disease.)... . these are footnote references
Also...other segment topics ...
Excess Calcium Promotes Cancer....
Excess Calcium & Toxins promote Increased Cellular Dysfunction and Death
Excess Calcium Increases Death Rate from All Diseases
The Toxicity of Calcium Supplementation
Calcium's Deadly Myths
Untangling Fact from Fiction
Myth #1 "Calcium supplementation and increased dietary calcium are good for you"
Myth #2 "You cannot get enough calcium in your diet without dairy products."
Myth #3 "Everyone with osteoporosis has a calcium deficiency"
(3 out of 8 elaborations)
Dr. Levy is not alone in presenting the risks of excess calcium in the body. Fortunately, there are many medical professionals giving similar advice and precautions based on the science. The problem is basically, that it's easy to get a lot of calcium from common dietary intake. Not so easy to get optimal magnesium... which has been a common focus here and should remain so as it definitely has an influence on excitability of cardiac cells and that's basic science.
Jackie
Death by Calcium
Thomas E. Levy, MD, JD
MedFox Publishing
Copyright 2013
|
Re: Can’t figure out the triggers August 24, 2018 01:07PM |
Registered: 9 years ago Posts: 182 |
Quote
Jackie
Beardman - your intake of calcium... I consume 1,000-1,500 MG of calcium a day is very high.
You need to cut back to under 500 mg or less... on a permanent basis. ... because calcium is excitatory to cells... that includes heart cells. And it will dominate over magnesium... (which is calming or relaxing)..... If your magnesium intake is consistently low, then that explains the problems you are experiencing. Most afibbers need to supplement with magnesium continually... especially those who are heavy exercisers.... and it needs to be the form of magnesium that reaches the interior of the cell without interference.
There is a book written by a cardiologist... Thomas E. Levy, MD, JD... titled Death by Calcium.... and he goes into all the details as to why calcium intake is so detrimental to the body on many levels. We need some calcium but not nearly the amount that many people take in daily.
Jackie
I wouldn't trust anything from Thomas Levy. He claims to be an expert on everything while hawking his supplements and books. For example, makes all kinds of unsubstantiated claims about Vitamin C and infectious diseases like Ebola, yet no publication record in support.
I would stop supplementing with Mg with your 35-40 bpm sleeping HR, or at least discuss first with an EP.
|
Re: Can’t figure out the triggers August 24, 2018 01:37PM |
Registered: 9 years ago Posts: 1,087 |
Beardman:
'My EP suggested that I take flecainide, but cautioned me that I absolutely couldn’t take it before the cardioversion as it could put me into NSR which could throw a clot. I know they are going by the book and I don’t want a stroke, but I just wish I could find the balance a little better."
Are you misunderstanding what your EP said? The whole point of taking a AAM like Flecainide is to convert to NSR, and avoid ECV's. Throw a Clot? the chances of that are much higher with an ECV, as the massive jolt from the Shock might dislodge a a Clot attached to the Wall of the Heart. Also, you are already Self-Converting 1-2 times a week anyway, why would your Dr. be extra concerned about Self-Conversion prior to a scheduled ECV? Iv'e had several times where I had an ECV scheduled while taking Flecainide, then in final hours before the ECV was to happen, I Self-Converted back to NSR. My EP and everyone was jubilant that I didn't need to follow through with the ECV. Maybe your Dr. wanted to have an TEE Echo done before the ECV, to check the Atria for Clots, but he could have ordered this without an ECV.
'My EP suggested that I take flecainide, but cautioned me that I absolutely couldn’t take it before the cardioversion as it could put me into NSR which could throw a clot. I know they are going by the book and I don’t want a stroke, but I just wish I could find the balance a little better."
Are you misunderstanding what your EP said? The whole point of taking a AAM like Flecainide is to convert to NSR, and avoid ECV's. Throw a Clot? the chances of that are much higher with an ECV, as the massive jolt from the Shock might dislodge a a Clot attached to the Wall of the Heart. Also, you are already Self-Converting 1-2 times a week anyway, why would your Dr. be extra concerned about Self-Conversion prior to a scheduled ECV? Iv'e had several times where I had an ECV scheduled while taking Flecainide, then in final hours before the ECV was to happen, I Self-Converted back to NSR. My EP and everyone was jubilant that I didn't need to follow through with the ECV. Maybe your Dr. wanted to have an TEE Echo done before the ECV, to check the Atria for Clots, but he could have ordered this without an ECV.
|
Re: Can’t figure out the triggers August 24, 2018 01:45PM |
Admin Registered: 6 years ago Posts: 5,351 |
I suspect he's being required to take anticoagulants for three weeks prior to the cardioversion to give any existing clots time to dissolve. That's standard procedure. So what his EP is saying is don't take flecainide until that time period has passed. You definitely don't want to convert to NSR by any means when you've got a clot lurking in your left atrium.
Another option would be to do a TEE to see if there is a clot, and if not going ahead with the cardioversion right away. That's what I would ask them to do.
Another option would be to do a TEE to see if there is a clot, and if not going ahead with the cardioversion right away. That's what I would ask them to do.
|
Re: Can’t figure out the triggers August 24, 2018 02:33PM |
Registered: 6 years ago Posts: 444 |
Quote
Jackie
Myth #1 "Calcium supplementation and increased dietary calcium are good for you"
Myth #2 "You cannot get enough calcium in your diet without dairy products."
Myth #3 "Everyone with osteoporosis has a calcium deficiency"
(3 out of 8 elaborations)
Dr. Levy is not alone in presenting the risks of excess calcium in the body. Fortunately, there are many medical professionals giving similar advice and precautions based on the science. The problem is basically, that it's easy to get a lot of calcium from common dietary intake.
Great, so don't take calcium supplements. I'm on a vegetarian diet, but like yogurt. There's a ton of research on what calcium does for you. I never subscribed to the listed myths.
(or I was for many years...lately I've added some Salmon and chicken).
Edited 1 time(s). Last edit at 08/24/2018 02:57PM by jpeters.
|
Re: Can’t figure out the triggers August 24, 2018 03:08PM |
Registered: 8 years ago Posts: 1,102 |
Quote
bolimasa
Thanks for the info.
And thanks for the new to me word - "prandially" I'd never heard that one before, and always enjoy an opportunity to learn a new word.
Your description makes me wonder if I am 'mixed'.
Certainly my medical test indicated Afib under exertion, Kinda makes me wonder if this relates to me being a "bad uphill girl" something I've struggled with my whole life. Has my heart always gone a little wacky when I hit that certain exertion point? I wish there was a way to know.
It would be easier to figure all this out if I could really tell when I am in afib... I also wonder about the vagal issue. One odd thing I've been trying to figure out is if there is a link between my pulsitile tinnitus and my afib... I started getting the pulsitile tinnitus ~ 2 years prior to my afib diagnosis. I don't have it all the time, or at least don't notice it all the time, but when I do hear it is when I rest on my couch in the evening and when I go to bed. Now I'm wondering if I am more afibby at this time. I have also noticed that of the few times I could really tell I am in afib, those events happened at night in bed.
Maybe none of this **really** matters... but maybe it would be good for me to understand my patterns (if they exist) so I can best assess my ablation recovery.
From what you've described - going into AF during the stress echo test - I'd say you're at least adrenergic and possibly "mixed".
It isn't really going to matter much to the EP ablationist. It doesn't change his strategy. My experience post-ablation is that if bad things are going to happen, they're going to happen differently than before anyway. It makes sense to me that if you've altered the electrical substrate of the atria with burns then it's going to behave differently afterwards. If you had an ablation and found yourself as symptomatic as before and with the same trigger patterns, I'd take that as a pretty strong indication that the ablation was a) PVI-only and b) not anwhere near transmural. In other words, a failure probably done by a less experienced operator. (Your EP, Dr. Marrouche, does not fit into this category so no worries there).
|
Re: Can’t figure out the triggers August 24, 2018 03:49PM |
Registered: 5 years ago Posts: 129 |
Quote
wolfpack
From what you've described - going into AF during the stress echo test - I'd say you're at least adrenergic and possibly "mixed".
It isn't really going to matter much to the EP ablationist. It doesn't change his strategy. My experience post-ablation is that if bad things are going to happen, they're going to happen differently than before anyway. It makes sense to me that if you've altered the electrical substrate of the atria with burns then it's going to behave differently afterwards. If you had an ablation and found yourself as symptomatic as before and with the same trigger patterns, I'd take that as a pretty strong indication that the ablation was a) PVI-only and b) not anwhere near transmural. In other words, a failure probably done by a less experienced operator. (Your EP, Dr. Marrouche, does not fit into this category so no worries there).
I'm certainly hoping my doc is as good as his reputation...
I feel pretty fortunate to have just lucked my way into having a good doctor.
Now I just need to figure out how to fix myself so I can keep it from coming back if I'm lucky enough to have a successful ablation.
|
Re: Can’t figure out the triggers August 24, 2018 07:44PM |
Registered: 5 years ago Posts: 45 |
Quote
The Anti-Fib
Beardman:
'My EP suggested that I take flecainide, but cautioned me that I absolutely couldn’t take it before the cardioversion as it could put me into NSR which could throw a clot. I know they are going by the book and I don’t want a stroke, but I just wish I could find the balance a little better."
Are you misunderstanding what your EP said? The whole point of taking a AAM like Flecainide is to convert to NSR, and avoid ECV's. Throw a Clot? the chances of that are much higher with an ECV, as the massive jolt from the Shock might dislodge a a Clot attached to the Wall of the Heart. Also, you are already Self-Converting 1-2 times a week anyway, why would your Dr. be extra concerned about Self-Conversion prior to a scheduled ECV? Iv'e had several times where I had an ECV scheduled while taking Flecainide, then in final hours before the ECV was to happen, I Self-Converted back to NSR. My EP and everyone was jubilant that I didn't need to follow through with the ECV. Maybe your Dr. wanted to have an TEE Echo done before the ECV, to check the Atria for Clots, but he could have ordered this without an ECV.
I confirmed with the EP multiple times to make sure I understood. As I understand it though it is a by the book play as I had been out of NSR for longer than 48 hours.
|
Re: Can’t figure out the triggers August 24, 2018 07:50PM |
Registered: 5 years ago Posts: 45 |
Quote
Carey
I suspect he's being required to take anticoagulants for three weeks prior to the cardioversion to give any existing clots time to dissolve. That's standard procedure. So what his EP is saying is don't take flecainide until that time period has passed. You definitely don't want to convert to NSR by any means when you've got a clot lurking in your left atrium.
Another option would be to do a TEE to see if there is a clot, and if not going ahead with the cardioversion right away. That's what I would ask them to do.
The plan was for a TEE and then a ECV, since my chads vasc score is zero it seemed than my stroke chances were actually higher while taking the meds the EP and other cardiologist wanted me on. The stroke chances also appeared to be higher having an ECV done as aposed to just waiting for me to naturally convert. The EP said that my stroke chances where the same no matter how the conversion occurred. He said it didn’t matter if it was an EVC, drug induced or naturally occurring. That statement just didn’t make sense to me and the statistics that I read after the fact didn’t seem to match up either. Again, I am not looking for a stroke, but it just seems like the advice being given is all based on liability.
|
Re: Can’t figure out the triggers August 24, 2018 08:03PM |
Registered: 5 years ago Posts: 45 |
Quote
Jackie
Beardman - your intake of calcium... I consume 1,000-1,500 MG of calcium a day is very high.
You need to cut back to under 500 mg or less... on a permanent basis. ... because calcium is excitatory to cells... that includes heart cells. And it will dominate over magnesium... (which is calming or relaxing)..... If your magnesium intake is consistently low, then that explains the problems you are experiencing. Most afibbers need to supplement with magnesium continually... especially those who are heavy exercisers.... and it needs to be the form of magnesium that reaches the interior of the cell without interference.
There is a book written by a cardiologist... Thomas E. Levy, MD, JD... titled Death by Calcium.... and he goes into all the details as to why calcium intake is so detrimental to the body on many levels. We need some calcium but not nearly the amount that many people take in daily.
Jackie
It just dawned upon me that when I was originally diagnosed I was eating a completely vegan diet so I can only figure that my calcium intake was almost if not zero. I will definitely be trying a drastic reduction in ca since it is an easy test. Thank you for the advice.
|
Re: Can’t figure out the triggers August 24, 2018 09:23PM |
Registered: 8 years ago Posts: 1,102 |
Quote
beardman
The plan was for a TEE and then a ECV, since my chads vasc score is zero it seemed than my stroke chances were actually higher while taking the meds the EP and other cardiologist wanted me on. The stroke chances also appeared to be higher having an ECV done as aposed to just waiting for me to naturally convert. The EP said that my stroke chances where the same no matter how the conversion occurred. He said it didn’t matter if it was an EVC, drug induced or naturally occurring. That statement just didn’t make sense to me and the statistics that I read after the fact didn’t seem to match up either. Again, I am not looking for a stroke, but it just seems like the advice being given is all based on liability.
Be careful to understand what the CHADSVasc score is telling you. A score of zero does not mean your stroke risk is zero. Nor does it mean your stroke risk is the same as it otherwise would be if you were in NSR. When you are in AF, your stroke risk is increased by 400%. What a CHADSVasc score of less than two means is there is “no net benefit” of anticoagulation. Anticoagulation, any kind, carries a risk of bleeding. So if you take the anticoagulation medicine, and your CHADSVasc score is a one or a zero then the risk of you suffering a bleed is greater than or equal to the risk of you having a stroke. The actual stroke risk, however, remains at four times what it was when you were in rhythm.
|
Re: Can’t figure out the triggers August 24, 2018 09:35PM |
Admin Registered: 6 years ago Posts: 5,351 |
Quote
beardman
The EP said that my stroke chances where the same no matter how the conversion occurred. He said it didn’t matter if it was an EVC, drug induced or naturally occurring.
Your EP is correct. The risk is that if there's a clot in your left atrium and you return to NSR, the resumed effective pumping action will pump the clot out and a stroke is the likely result. It doesn't matter how or why you returned to NSR.
Frankly, I don't understand what the issue is here if your EP planned on a TEE prior to the cardioversion. Do the TEE and cardioversion and be done with it.
|
Re: Can’t figure out the triggers August 24, 2018 10:08PM |
Registered: 8 years ago Posts: 1,102 |
|
Re: Can’t figure out the triggers August 25, 2018 12:47AM |
Registered: 6 years ago Posts: 444 |
Quote
beardman
Beardman - your intake of calcium... I consume 1,000-1,500 MG of calcium a day is very high.
You need to cut back to under 500 mg or less... on a permanent basis. ... because calcium is excitatory to cells... that includes heart cells. And it will dominate over magnesium... (which is calming or relaxing)..... If your magnesium intake is consistently low, then that explains the problems you are experiencing. Most afibbers need to supplement with magnesium continually... especially those who are heavy exercisers.... and it needs to be the form of magnesium that reaches the interior of the cell without interference.
There is a book written by a cardiologist... Thomas E. Levy, MD, JD... titled Death by Calcium.... and he goes into all the details as to why calcium intake is so detrimental to the body on many levels. We need some calcium but not nearly the amount that many people take in daily.
Jackie
It just dawned upon me that when I was originally diagnosed I was eating a completely vegan diet so I can only figure that my calcium intake was almost if not zero. I will definitely be trying a drastic reduction in ca since it is an easy test. Thank you for the advice.
Let's hope that you didn't understand what she was saying. If you're on a strictly vegan diet, you especially need to make sure you're getting enough calcium.
"Calcium and the heart: a question of life and death. ... The importance of calcium-dependent signaling in the heart has been appreciated for decades. For example, it is well accepted that intracellular calcium release from the sarcoplasmic reticulum (SR) is required for cardiac muscle contraction."
Edited 2 time(s). Last edit at 08/25/2018 01:11AM by jpeters.
|
Re: Can’t figure out the triggers August 25, 2018 04:14AM |
Registered: 9 years ago Posts: 1,087 |
Quote
beardman
Carey said:
I suspect he's being required to take anticoagulants for three weeks prior to the cardioversion to give any existing clots time to dissolve. That's standard procedure. So what his EP is saying is don't take flecainide until that time period has passed. You definitely don't want to convert to NSR by any means when you've got a clot lurking in your left atrium.
Another option would be to do a TEE to see if there is a clot, and if not going ahead with the cardioversion right away. That's what I would ask them to do.
_______________________________________________________________________________________________
The plan was for a TEE and then a ECV, since my chads vasc score is zero it seemed than my stroke chances were actually higher while taking the meds the EP and other cardiologist wanted me on. The stroke chances also appeared to be higher having an ECV done as aposed to just waiting for me to naturally convert. The EP said that my stroke chances where the same no matter how the conversion occurred. He said it didn’t matter if it was an EVC, drug induced or naturally occurring. That statement just didn’t make sense to me and the statistics that I read after the fact didn’t seem to match up either. Again, I am not looking for a stroke, but it just seems like the advice being given is all based on liability.
Really you are correct Beardman. ECV is not warranted. Why ECV when in, a day or 2 later you covert on your own, and then 3 days later your back in AFIB. BTW, the biggest risk of an ECV for would probably from the Anesthesia. Your Doctor is giving you generic advice and totally discounting what you are saying about going in and out of AFIB. This is not uncommon, as Dr's dont always trust patients accounts of when their in AFIB, or NSR. Maybe he has some Theory he wants to test, that giving a blast of Electricity may somehow help the situation. In any regards I would get another opinion and try another Dr.
|
Re: Can’t figure out the triggers August 25, 2018 04:35AM |
Registered: 12 years ago Posts: 247 |
I’m with Jackie on the Calcium. We certainly don’t need a huge amount to be in the healthy range. In fact I stopped taking it at all after being told I had Osteoporosis...having been supplementing with it for 20 years.
My bone doc suggested high dose D3 and calcium from natural sources, but don’t overdo it. So it’s yogurt, full cream milk, bit of cheese and as a vegetarian, plenty of veggies nuts pulses etc.
Calcium is also contraindicated in regards to heart disease.
My last bone density was better , so small steps.
My bone doc suggested high dose D3 and calcium from natural sources, but don’t overdo it. So it’s yogurt, full cream milk, bit of cheese and as a vegetarian, plenty of veggies nuts pulses etc.
Calcium is also contraindicated in regards to heart disease.
My last bone density was better , so small steps.
|
Re: Can’t figure out the triggers August 25, 2018 05:03AM |
Registered: 9 years ago Posts: 1,087 |
Quote
beardman
Beardman:
'My EP suggested that I take flecainide, but cautioned me that I absolutely couldn’t take it before the cardioversion as it could put me into NSR which could throw a clot. I know they are going by the book and I don’t want a stroke, but I just wish I could find the balance a little better."
_______________________________________________________________________________________________
Anti-FIB:
Are you misunderstanding what your EP said? The whole point of taking a AAM like Flecainide is to convert to NSR, and avoid ECV's. Throw a Clot? the chances of that are much higher with an ECV, as the massive jolt from the Shock might dislodge a a Clot attached to the Wall of the Heart. Also, you are already Self-Converting 1-2 times a week anyway, why would your Dr. be extra concerned about Self-Conversion prior to a scheduled ECV? Iv'e had several times where I had an ECV scheduled while taking Flecainide, then in final hours before the ECV was to happen, I Self-Converted back to NSR. My EP and everyone was jubilant that I didn't need to follow through with the ECV. Maybe your Dr. wanted to have an TEE Echo done before the ECV, to check the Atria for Clots, but he could have ordered this without an ECV.
______________________________________________________________________________________________
Beardman:
I confirmed with the EP multiple times to make sure I understood. As I understand it though it is a by the book play as I had been out of NSR for longer than 48 hours.
So your EP is saying that if a patient has been in AFIB>48 hours, that they must discontinue Anti-Arrthmics, as it it might convert them back to NSR, thus causing Stroke. An then the Patient undergoes TEE/ECV to get back to NSR.
If such a treatment protocol exists, someone please direct me to it. I've been in these scenarios many times, having 30 ECV's. Sure getting out of AFIB<48 hours is the Goal, but to suggest that we should avoid spontaneous self-conversions by withholding AAM's is new to me. At some point you have to try and get out of AFIB, it's not risk free.
In your case, it sounds like you've Already had 50+ self-conversions over the last year. This is why minimizing Stroke risk is important, and Dr's emphasize anti-coagulation especially for someone in out out of AFIB as much as you are.
|
Re: Can’t figure out the triggers August 25, 2018 08:46AM |
Registered: 5 years ago Posts: 45 |
Quote
The Anti-Fib
Beardman:
'My EP suggested that I take flecainide, but cautioned me that I absolutely couldn’t take it before the cardioversion as it could put me into NSR which could throw a clot. I know they are going by the book and I don’t want a stroke, but I just wish I could find the balance a little better."
_______________________________________________________________________________________________
Anti-FIB:
Are you misunderstanding what your EP said? The whole point of taking a AAM like Flecainide is to convert to NSR, and avoid ECV's. Throw a Clot? the chances of that are much higher with an ECV, as the massive jolt from the Shock might dislodge a a Clot attached to the Wall of the Heart. Also, you are already Self-Converting 1-2 times a week anyway, why would your Dr. be extra concerned about Self-Conversion prior to a scheduled ECV? Iv'e had several times where I had an ECV scheduled while taking Flecainide, then in final hours before the ECV was to happen, I Self-Converted back to NSR. My EP and everyone was jubilant that I didn't need to follow through with the ECV. Maybe your Dr. wanted to have an TEE Echo done before the ECV, to check the Atria for Clots, but he could have ordered this without an ECV.
______________________________________________________________________________________________
Beardman:
I confirmed with the EP multiple times to make sure I understood. As I understand it though it is a by the book play as I had been out of NSR for longer than 48 hours.
So your EP is saying that if a patient has been in AFIB>48 hours, that they must discontinue Anti-Arrthmics, as it it might convert them back to NSR, thus causing Stroke. An then the Patient undergoes TEE/ECV to get back to NSR.
If such a treatment protocol exists, someone please direct me to it. I've been in these scenarios many times, having 30 ECV's. Sure getting out of AFIB<48 hours is the Goal, but to suggest that we should avoid spontaneous self-conversions by withholding AAM's is new to me. At some point you have to try and get out of AFIB, it's not risk free.
In your case, it sounds like you've Already had 50+ self-conversions over the last year. This is why minimizing Stroke risk is important, and Dr's emphasize anti-coagulation especially for someone in out out of AFIB as much as you are.
This was on my initial visit to the EP. I was not at that time and am still not on any medication. He wanted to have me undergo an ECV the following day and wanted me to start a blood thinner immediately. He didn’t want me taking the flecanide before since he said I would have only been on the thinner for a day. He said if I self converted before the ECV then I could start taking it.
I know the past is the past, but the only thing all the different cardiologist and the EP seem to agree on is that I have had this most likely my entire life or at least since my early 20’s (I am only 36 now). I have such a hard time understanding or believing that this has been having for so long and that NOW I need to take all these drugs or have an ablation. I just don’t trust having to be on pharmaceuticals for the next 40 years. Especially since with some adjustments to my life I have already been able to go from 4-5 week boughts of being out of NSR to 1-2 days.
I can’t help thinking that, “my case is different”. Maybe it is, maybe it isn’t.
|
Re: Can’t figure out the triggers August 25, 2018 12:15PM |
Registered: 6 years ago Posts: 18,881 |
Yes - JoyWin - that's smart. Good for you.
For those on vegan diets, there is more than abundant calcium content in the vegan foods to satisfy the body’s requirements so avoiding dairy isn't really a penalty that requires supplementation with extra calcium. The risks of too much calcium and especially in afibbers is real and correct from a basic, biochemistry standpoint.
That's why calcium channel blockers seem to be helpful in patients... they block the contracting of muscles in heart and arteries when there is excess calcium. However, some forward-thinking doctors have asked...if you block the calcium, where does the excess calcium go? It gets deposited into arteries ... according to a paper presented at European Cardiology Society in Amsterdam noting CCBs caused 85,000 avoidable heart attacks and cases of heart failure each year.
Very early in my AF years, I was taking supplemental calcium as directed by my GP as advice for post-menopausal women. I found an association between when I took the calcium supplement and onset of afib...so it was an obvious message to stop the Ca supplements and that definitely helped. Then, several years later, I found this forum and became acquainted with "the magnesium factor" as it relates to AF.
There is misguided concern about the need for calcium for strong bones. Yes, calcium is one component but there are a total of 76 minerals needed for proper bone health and strength... and calcium is only one and they all need to be in proper balance and ratio.
Jackie
For those on vegan diets, there is more than abundant calcium content in the vegan foods to satisfy the body’s requirements so avoiding dairy isn't really a penalty that requires supplementation with extra calcium. The risks of too much calcium and especially in afibbers is real and correct from a basic, biochemistry standpoint.
That's why calcium channel blockers seem to be helpful in patients... they block the contracting of muscles in heart and arteries when there is excess calcium. However, some forward-thinking doctors have asked...if you block the calcium, where does the excess calcium go? It gets deposited into arteries ... according to a paper presented at European Cardiology Society in Amsterdam noting CCBs caused 85,000 avoidable heart attacks and cases of heart failure each year.
Very early in my AF years, I was taking supplemental calcium as directed by my GP as advice for post-menopausal women. I found an association between when I took the calcium supplement and onset of afib...so it was an obvious message to stop the Ca supplements and that definitely helped. Then, several years later, I found this forum and became acquainted with "the magnesium factor" as it relates to AF.
There is misguided concern about the need for calcium for strong bones. Yes, calcium is one component but there are a total of 76 minerals needed for proper bone health and strength... and calcium is only one and they all need to be in proper balance and ratio.
Jackie
|
Re: Can’t figure out the triggers August 25, 2018 12:30PM |
Registered: 6 years ago Posts: 18,881 |
safib - The referenced calcium studies in the Death by Calcium book are not Dr. Levy's pipe dreams.
As I commented to JoyWin in another post, the risks of too much calcium and especially in afibbers is real and correct from a basic, biochemistry standpoint and is supported by not only those fundamentals, but also the studies showing the excitatory effect on muscle cells including heart cells.
That said... It's appropriate to question anything that seems too good to be true.. I always do that myself; but let me tell you... the high-dose vitamin C Dr. Levy touts in his other books are both useful and help prevent and reverse many ailments not managed easily by other conventional meds.
If you haven't experienced the awesome efficacy of using Liposomal Vitamin C to ward off the onset of a cold or flu, for example, you've really missed something amazing. That form provides the ease of taking very high doses of vitamin C that typically would not be tolerated (bowel) in a short period of time with regular C. I've used it; family has used it; friends are amazed and I know afibbers who would never want to be without it... esp. when traveling.
Dr. Levy isn't the only one touting the benefits of the liposomal delivery system of nutrients. And, of course, there is a huge amount of history on the basic, preventive and curing effects of vitamin C.
Jackie
As I commented to JoyWin in another post, the risks of too much calcium and especially in afibbers is real and correct from a basic, biochemistry standpoint and is supported by not only those fundamentals, but also the studies showing the excitatory effect on muscle cells including heart cells.
That said... It's appropriate to question anything that seems too good to be true.. I always do that myself; but let me tell you... the high-dose vitamin C Dr. Levy touts in his other books are both useful and help prevent and reverse many ailments not managed easily by other conventional meds.
If you haven't experienced the awesome efficacy of using Liposomal Vitamin C to ward off the onset of a cold or flu, for example, you've really missed something amazing. That form provides the ease of taking very high doses of vitamin C that typically would not be tolerated (bowel) in a short period of time with regular C. I've used it; family has used it; friends are amazed and I know afibbers who would never want to be without it... esp. when traveling.
Dr. Levy isn't the only one touting the benefits of the liposomal delivery system of nutrients. And, of course, there is a huge amount of history on the basic, preventive and curing effects of vitamin C.
Jackie
|
Re: Can’t figure out the triggers August 25, 2018 12:31PM |
Registered: 6 years ago Posts: 706 |
|
Re: Can’t figure out the triggers August 25, 2018 12:37PM |
Registered: 6 years ago Posts: 444 |
Quote
Jackie
However, some forward-thinking doctors have asked...if you block the calcium, where does the excess calcium go? It gets deposited into arteries ... according to a paper presented at European Cardiology Society in Amsterdam noting CCBs caused 85,000 avoidable heart attacks and cases of heart failure each year.
Interesting. I've read just the opposite.
"Calcium channel blockers, also called calcium antagonists, decrease the rate at which calcium flows into the heart and blood vessel walls. This, says Zanchetti, appears to have the beneficial effect of slowing the growth of cells that line the blood vessels and arteries and reducing the size of plaques, the fat deposits that accumulate in arteries. "
[www.sciencedaily.com]
|
Re: Can’t figure out the triggers August 25, 2018 12:49PM |
Registered: 6 years ago Posts: 444 |
Quote
Jackie
For those on vegan diets, there is more than abundant calcium content in the vegan foods to satisfy the body’s requirements so avoiding dairy isn't really a penalty that requires supplementation with extra calcium. The risks of too much calcium and especially in afibbers is real and correct from a basic, biochemistry standpoint.
They can probably get all they need from fruits and vegetables. No need for supplements. That's a lot different from saying people don't need calcium (you didn't). The exact requirement is unknown, so you can't quote a number that's right for everyone.
Scary article on calcium channel blockers:
"Blocking the flow of calcium is dangerous since calcium is essential for normal cell life and operation – as well as for the whole body. Without sufficient calcium, you cannot live."
[www.justlivewell.com]
Edited 2 time(s). Last edit at 08/25/2018 01:05PM by jpeters.
|
Re: Can’t figure out the triggers August 25, 2018 01:54PM |
Registered: 6 years ago Posts: 920 |
As I wrote in a couple of threads, I've frequent but short afib episodes.
I'm supplementing with Mg bisglycinate, I've still afib, but better sleep.
Since two days, I've started cutting on my calcium consumption. I like cheese and dairy products, so I've banned them for a moment. I'll see if it does something...
(I've already done this, but back then, I wasn't supplementing with Mg.)
I'm supplementing with Mg bisglycinate, I've still afib, but better sleep.
Since two days, I've started cutting on my calcium consumption. I like cheese and dairy products, so I've banned them for a moment. I'll see if it does something...
(I've already done this, but back then, I wasn't supplementing with Mg.)
|
Re: Can’t figure out the triggers August 25, 2018 02:27PM |
Admin Registered: 6 years ago Posts: 5,351 |
Quote
jpeters
Scary article on calcium channel blockers:
Until you notice that the newest research they relied on to arrive at the scary article is 18 years old and contradicted by larger, more recent studies. For example:
Quote
CONCLUSION:
Our study demonstrates that CCBs reduce the risk of all-cause mortality compared with active therapy and prevent heart failure compared with placebo. Furthermore, with the inclusion of recent trials, we confirm that they reduce the risk of stroke, also in comparison to angiotensin-converting enzyme inhibitors and do not increase the risk of cardiovascular death, myocardial infarction and major cardiovascular events.
And:
Quote
Conclusions This large population-based study provides strong evidence that CCB use is not associated with an increased risk of cancer. The analyses yielded robust results across all types of cancer and different durations of exposure to CCBs.
|
Re: Can’t figure out the triggers August 25, 2018 02:43PM |
Registered: 6 years ago Posts: 444 |
Quote
Carey
Scary article on calcium channel blockers:
Until you notice that the newest research they relied on to arrive at the scary article is 18 years old and contradicted by larger, more recent studies. For example:
Yours is from 2009
 I assume they have a beneficial role (lowering mortality) and am glad they don't cause cancer (I'm currently taking some diltiazem). The quoted article was more about the importance of getting enough calcium..which probably hasn't changed much in the last 18 years.
I assume they have a beneficial role (lowering mortality) and am glad they don't cause cancer (I'm currently taking some diltiazem). The quoted article was more about the importance of getting enough calcium..which probably hasn't changed much in the last 18 years.Edited 2 time(s). Last edit at 08/25/2018 02:50PM by jpeters.
|
Re: Can’t figure out the triggers August 25, 2018 04:51PM |
Registered: 11 years ago Posts: 4,226 |
Do you need calcium, yes. You just don't need too much. I took the dairy consumption data and hip fracture incidence from this table <[www.nature.com] and plotted them. It this associational, yes. But since dairy is a big source of calcium, it is reasonable to do. Years before I recall seeing that countries with calcium intakes/day <500mg had some of the lowest hip fracture rates.. Are there other variables, certainly. In my wife's and my case, we get around 600 mg/day. We aren't vegan but consume no dairy. In Sept 2017 we did DEXA bone density scans. I have a t-score of 0.3 and she's a 0.9. A positive t score is how many standard deviations your bone density is above the mean for a person of your sex at age 30. I'm 63 and my wife is 58.
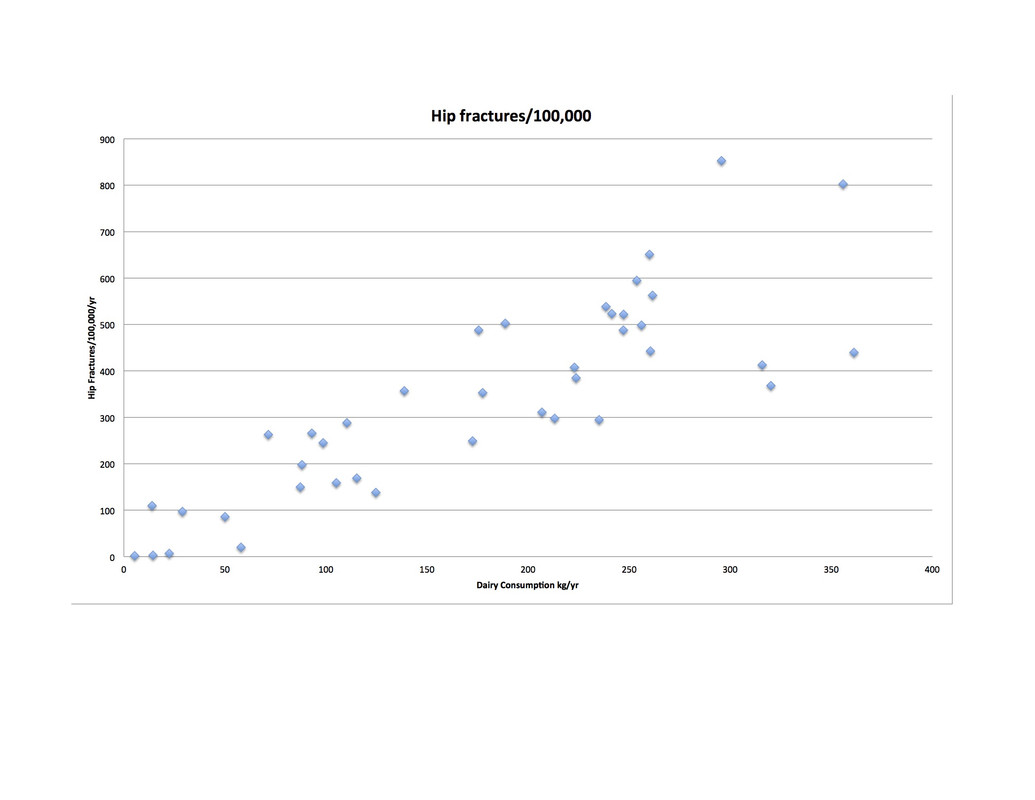
Here are the top 8
Hip fractures/100,000 Dairy kg/yr
Denmark 853 295.62
Sweden 802.8 355.86
Kazakhstan 651.1 260
United States 595 253.8
Norway 563 261.52
Belgium 538.7 238.47
United Kingdom 523.5 241.47
Germany 522 247.24
Here are the top 8
Hip fractures/100,000 Dairy kg/yr
Denmark 853 295.62
Sweden 802.8 355.86
Kazakhstan 651.1 260
United States 595 253.8
Norway 563 261.52
Belgium 538.7 238.47
United Kingdom 523.5 241.47
Germany 522 247.24
|
Re: Can’t figure out the triggers August 25, 2018 05:18PM |
Registered: 6 years ago Posts: 444 |
Did you factor out income, protein, and lactose persistence? Also, dairy consumption is different than calcium intake. There are also lots of other variables associated with wealthier countries. One other thing, there are probably over 60 factors that contribute to hip replacements, least of which would be consuming dairy. Nice job, though
Edited 1 time(s). Last edit at 08/25/2018 05:22PM by jpeters.
Edited 1 time(s). Last edit at 08/25/2018 05:22PM by jpeters.
|
Re: Can’t figure out the triggers August 25, 2018 08:25PM |
Registered: 5 years ago Posts: 45 |
Quote
The Anti-Fib
Did you ever follow up on an Endocrine/Cortisol check-up, as suggested in in your earlier Post? A Saliva Cortisol 4X/day test would tell what is going on with Adrenal output. The fact that you can sense it coming on several hours prior suggests some sort of intermittent Hormonal or Electrolytic imbalance. I had intermittent periods of Adrenal Suppression which triggered AFIB. I felt wiped out and unsually tired for about a day prior to my episodes.
Finally getting a chance to post this up, everything is elevated.

Also, went out of NSR this morning during a karate workout (not the norm at all). Didn’t get a chance to get on the bike today, but hopeful that tomorrow am at the gym with snap me back into NSR.
I understand that everyone is different and things effect people differently. I just wish I could find a doctor willing to work through it with me rather than prescribe pharmaceuticals or do an ablation. I guess we are our own doctors. Thank you so very much to everyone for their insights, I really do appreciate it.
|
Re: Can’t figure out the triggers August 26, 2018 12:22AM |
Registered: 9 years ago Posts: 1,087 |
Beardman:
I think every Dr. will want you on Blood Thinners. If it was only an episode every 2 months, then they would be more inclined to accept no Anti-Coagulation. Keep in mind when you are doing your research, that Paroximal AFIB could mean bi-monthly episodes, or 1-2 a week like yours.
The other thing is that you are relatively early in your discovery of your AFIB. You have done well and better than most in understanding this complex condition you have. Patience is warranted here. I still think you should medicate during episodes, and I stand by my post regarding this in your initial Thread several months ago.
I think every Dr. will want you on Blood Thinners. If it was only an episode every 2 months, then they would be more inclined to accept no Anti-Coagulation. Keep in mind when you are doing your research, that Paroximal AFIB could mean bi-monthly episodes, or 1-2 a week like yours.
The other thing is that you are relatively early in your discovery of your AFIB. You have done well and better than most in understanding this complex condition you have. Patience is warranted here. I still think you should medicate during episodes, and I stand by my post regarding this in your initial Thread several months ago.
|
Re: Can’t figure out the triggers August 26, 2018 08:48AM |
Registered: 5 years ago Posts: 45 |
Quote
The Anti-Fib
Beardman:
I think every Dr. will want you on Blood Thinners. If it was only an episode every 2 months, then they would be more inclined to accept no Anti-Coagulation. Keep in mind when you are doing your research, that Paroximal AFIB could mean bi-monthly episodes, or 1-2 a week like yours.
The other thing is that you are relatively early in your discovery of your AFIB. You have done well and better than most in understanding this complex condition you have. Patience is warranted here. I still think you should medicate during episodes, and I stand by my post regarding this in your initial Thread several months ago.
I understand am trying to be patient with this, but as you all know it is tough. It is especially difficult for me when I appear to be doing to same thing and am receiving different results. I keep a journal of everything that I can think relates to this. My new things to make note of will be the calcium intake also any association with bradycardia and perhaps Hawthorne berry (Iv’e been doing a fair amount of reading on that as well).
From an outside point of view I don’t disagree with the medication. They would have just such a huge impact on my life being that they want me to stop any martial arts at all while on the blood thinners. On top of this, it seems that the pharmaceuticals are only a temporary solution for most people, especially when their younger. Oh, and then their is the huge cost as well. I requested a blood thinner that had a reversal agent, apparently that is only Pradaxa. It would cost around $600/month just for that. I think the flecainide was another $150 or so and I am supposed to take that twice daily everyday.
|
Re: Can’t figure out the triggers August 26, 2018 10:16AM |
Registered: 8 years ago Posts: 1,102 |
Completely understand the frustration. Bear in mind, though, that we are all biologics and not machines. The same set of inputs does not always have to produce the same set of outputs. AF is a progressive disease. It will change over time. As things are today, there are really 3 choices for AF: don’t treat, medicate, ablate.
Eliquis has a reversal agent that was recently approved. It is called Andexxa. Your physician may not be aware of it yet. I’m not sure if there’s a big cost difference with respect to Pradaxa, though. It would be worth asking.
Eliquis has a reversal agent that was recently approved. It is called Andexxa. Your physician may not be aware of it yet. I’m not sure if there’s a big cost difference with respect to Pradaxa, though. It would be worth asking.
|
Re: Can’t figure out the triggers August 26, 2018 11:16AM |
Registered: 5 years ago Posts: 45 |
Quote
wolfpack
Completely understand the frustration. Bear in mind, though, that we are all biologics and not machines. The same set of inputs does not always have to produce the same set of outputs. AF is a progressive disease. It will change over time. As things are today, there are really 3 choices for AF: don’t treat, medicate, ablate.
Eliquis has a reversal agent that was recently approved. It is called Andexxa. Your physician may not be aware of it yet. I’m not sure if there’s a big cost difference with respect to Pradaxa, though. It would be worth asking.
I will check out Eliquis so that maybe I have another option, thank you.
Kind of just had an aha moment this morning and feel like a real idiot. My bp is right around 105/70, but that is only due to me increasing my sodium intake years ago. It used to be 90/60 or so (that was also when I was MUCH heavier). I just looked through my notes and my sodium intake has been in the 2000-2,500mg range daily for years. I don’t know why this never dawned upon me before. All my blood tests have always been normal, but this must be having an impact, I would think especially with my potassium balance, no?
With the three different cardiologists and the EP that I saw, not one of them even asked about my diet. I was very clear with all of them that I kept very good records of everything and even asked if changes in my diet might help. I always received the blanket statement that eating better is always good for you . . . What is,”better” when you don’t know what I’m eating! Sorry for the vent.
I’m have cut my ca intake down to 200-300mg
I have discontinued L-arginine
I am going to taper my sodium intake down and increase my K intake up.
We shall see
|
Re: Can’t figure out the triggers August 26, 2018 01:55PM |
Admin Registered: 6 years ago Posts: 5,351 |
Quote
beardman
With the three different cardiologists and the EP that I saw, not one of them even asked about my diet. I was very clear with all of them that I kept very good records of everything and even asked if changes in my diet might help. I always received the blanket statement that eating better is always good for you . . . What is,”better” when you don’t know what I’m eating! Sorry for the vent.
Actually, I somewhat understand their attitude. I've seen hundreds and hundreds of posts on multiple forums over the years from people who do various things with diet and supplements to try and manage their afib. Nothing stands out consistently as being truly helpful. Now imagine EPs who've seen thousands of afib patients and heard almost every one of them ask questions like that. What else can they say when they know there is no particular diet or supplement that will help everyone, or even most people? So they fall back on all they really can say with certainty: eating a healthy, balanced diet is always smart. It may not do a damn thing for your afib, but it won't make it worse.
|
Re: Can’t figure out the triggers August 26, 2018 03:45PM |
Registered: 10 years ago Posts: 1,748 |
Beardman:
You bet diet is very important, actually salt is necessary as well. Sea salt is what you should take as it has minerals. People do not feel well when sodium levels are lowered, their energy level drops and they develop hormonal and immune system imbalances. I also take magnesium, not a lot, but some everyday, years ago I used to have pacs which mag. stopped.
Most doctors don't want to listen about diet as that isn't their business, they are in the business of handing out pills or (slash and burn) not trying to find out what is causing your problems. I have had episodes of AF off and on for almost 20 years, magnesium has helped as has my diet. I grow most of my veggies and fruits, I eat nuts, chicken, some beef and fish, I work hard which is my exercise do not drink or smoke. Don't tell me that what you eat and the exercise you get isn't helpful towards your AF.
Liz
You bet diet is very important, actually salt is necessary as well. Sea salt is what you should take as it has minerals. People do not feel well when sodium levels are lowered, their energy level drops and they develop hormonal and immune system imbalances. I also take magnesium, not a lot, but some everyday, years ago I used to have pacs which mag. stopped.
Most doctors don't want to listen about diet as that isn't their business, they are in the business of handing out pills or (slash and burn) not trying to find out what is causing your problems. I have had episodes of AF off and on for almost 20 years, magnesium has helped as has my diet. I grow most of my veggies and fruits, I eat nuts, chicken, some beef and fish, I work hard which is my exercise do not drink or smoke. Don't tell me that what you eat and the exercise you get isn't helpful towards your AF.
Liz
|
Re: Can’t figure out the triggers August 26, 2018 04:09PM |
Registered: 6 years ago Posts: 444 |
Quote
Elizabeth
Most doctors don't want to listen about diet as that isn't their business, they are in the business of handing out pills or (slash and burn) not trying to find out what is causing your problems.
Liz
Yes, that's what worked. I've always maintained a very healthy lifestyle, but got afib anyway. Some slash and burn better than others. None really cared what caused it.
|
Re: Can’t figure out the triggers August 26, 2018 08:43PM |
Registered: 9 years ago Posts: 1,087 |
Quote
beardman
Beardman:
I think every Dr. will want you on Blood Thinners. If it was only an episode every 2 months, then they would be more inclined to accept no Anti-Coagulation. Keep in mind when you are doing your research, that Paroximal AFIB could mean bi-monthly episodes, or 1-2 a week like yours.
The other thing is that you are relatively early in your discovery of your AFIB. You have done well and better than most in understanding this complex condition you have. Patience is warranted here. I still think you should medicate during episodes, and I stand by my post regarding this in your initial Thread several months ago.
I understand am trying to be patient with this, but as you all know it is tough. It is especially difficult for me when I appear to be doing to same thing and am receiving different results. I keep a journal of everything that I can think relates to this. My new things to make note of will be the calcium intake also any association with bradycardia and perhaps Hawthorne berry (Iv’e been doing a fair amount of reading on that as well).
From an outside point of view I don’t disagree with the medication. They would have just such a huge impact on my life being that they want me to stop any martial arts at all while on the blood thinners. On top of this, it seems that the pharmaceuticals are only a temporary solution for most people, especially when their younger. Oh, and then their is the huge cost as well. I requested a blood thinner that had a reversal agent, apparently that is only Pradaxa. It would cost around $600/month just for that. I think the flecainide was another $150 or so and I am supposed to take that twice daily everyday.
If you just take Flecainide during an Episode, then you wouldn't need to use very much, especially if it shortens the event. I don't know where your at, but I think Flec is cheap in the US. If you can shorten your episodes down, then all of the other risks will be minimized. The issues with Stroke risk and TachyCardia induced Heart Failure, etc.
|
Re: Can’t figure out the triggers August 30, 2018 09:45AM |
Registered: 5 years ago Posts: 38 |
Hi Beardman-
I'm sorry you have to deal with this and understand it all too well. I just turned 45 so now how it is to get this diagnosis and feel like your life is in flux to say the least. Take the time to do some more reading, and I think you will likely conclude that an ablation is the way to go. You are young with a structurally sound heart so your success rate with a top EP will be very high. This is the best method of trying to get off these meds, at least temporarily. I've seen lots of people in your age group with years of med free NSR after a successful ablation. You will of course need to continue not to over-exercise and watch all of the other lifestyle factors- but that doesn't seem to be an issue for you. I don't see why you can't do martial arts on a blood thinner. If it's high contact then yes you might be banged up with bruises. The biggest risk would be hits to the head which hopefully isn't part of the protocol. I am snowboarding on a blood thinner. I don't go out on icy days, wear my helmet, and have a medical ID on me. My top EP advised me that the biggest risk is a bad head injury, and if you have one you'd be in trouble even if not on a blood thinner. I'm choosing to live my life with this diagnosis and try to accept it and move on. You are new to this and all of that will take time. But know that you can still do the things you love and will get through this.
Tracy
I'm sorry you have to deal with this and understand it all too well. I just turned 45 so now how it is to get this diagnosis and feel like your life is in flux to say the least. Take the time to do some more reading, and I think you will likely conclude that an ablation is the way to go. You are young with a structurally sound heart so your success rate with a top EP will be very high. This is the best method of trying to get off these meds, at least temporarily. I've seen lots of people in your age group with years of med free NSR after a successful ablation. You will of course need to continue not to over-exercise and watch all of the other lifestyle factors- but that doesn't seem to be an issue for you. I don't see why you can't do martial arts on a blood thinner. If it's high contact then yes you might be banged up with bruises. The biggest risk would be hits to the head which hopefully isn't part of the protocol. I am snowboarding on a blood thinner. I don't go out on icy days, wear my helmet, and have a medical ID on me. My top EP advised me that the biggest risk is a bad head injury, and if you have one you'd be in trouble even if not on a blood thinner. I'm choosing to live my life with this diagnosis and try to accept it and move on. You are new to this and all of that will take time. But know that you can still do the things you love and will get through this.
Tracy
|
Re: Can’t figure out the triggers September 01, 2018 06:35AM |
Registered: 5 years ago Posts: 45 |
Quote
Dinodog
Hi Beardman-
I'm sorry you have to deal with this and understand it all too well. I just turned 45 so now how it is to get this diagnosis and feel like your life is in flux to say the least. Take the time to do some more reading, and I think you will likely conclude that an ablation is the way to go. You are young with a structurally sound heart so your success rate with a top EP will be very high. This is the best method of trying to get off these meds, at least temporarily. I've seen lots of people in your age group with years of med free NSR after a successful ablation. You will of course need to continue not to over-exercise and watch all of the other lifestyle factors- but that doesn't seem to be an issue for you. I don't see why you can't do martial arts on a blood thinner. If it's high contact then yes you might be banged up with bruises. The biggest risk would be hits to the head which hopefully isn't part of the protocol. I am snowboarding on a blood thinner. I don't go out on icy days, wear my helmet, and have a medical ID on me. My top EP advised me that the biggest risk is a bad head injury, and if you have one you'd be in trouble even if not on a blood thinner. I'm choosing to live my life with this diagnosis and try to accept it and move on. You are new to this and all of that will take time. But know that you can still do the things you love and will get through this.
Tracy
Thank you for the response, I feel like a lot of the time this forum is as much a support group as it is an information resource. Since dropping my Ca levels down and stopping the L-Arginine I have noticed an interesting response. I modified my diet last weekend and it took me until karate on Tuesday to get back in NSR. Having said that though, I have been in rhythm since then with the exception of yesterday. Yesterday my resting hr was 50 and while running around work I noticed what seemed like a few PAC’s. I checked and I was out of NSR, about a minute later I was back in NSR. The same thing happened two more times yesterday afternoon. This may be normal for most of you all, but for me, once I’m out of NSR, I don’t go back in without a workout 99% of the time.
Regarding the anti-coagulation meds, yes, all the different cardiologists were concerned about head injuries. The biggest thing I think that scared me away from any meds was that everyone seemed to have their own different spin that was counterintelligent to the last guy. I know everyone is different and there is more than one way to skin a cat, but it just didn’t give me that comfortable feeling.
For right now, I have a couple of herniated/sequestered discs to deal with so hopefully the diet changes can make s difference.
|
Re: Can’t figure out the triggers September 01, 2018 08:19AM |
Registered: 8 years ago Posts: 1,102 |
|
Re: Can’t figure out the triggers September 01, 2018 08:51AM |
Registered: 6 years ago Posts: 18,881 |
Beardman - The support factor is definitely an important part of the forum. Always has been. I'm pleased to see your cutting back on the Ca and arginine helped and as time goes on, you'll probably see continued stability but you also may need further reductions. What are the numbers of the herniated discs?
Jackie
Jackie
|
Re: Can’t figure out the triggers September 01, 2018 08:57AM |
Registered: 5 years ago Posts: 45 |
Quote
Jackie
Beardman - The support factor is definitely an important part of the forum. Always has been. I'm pleased to see your cutting back on the Ca and arginine helped and as time goes on, you'll probably see continued stability but you also may need further reductions. What are the numbers of the herniated discs?
Jackie
Hoping for a microdiscectomy around L5, but it looks like at least L4 too. I’m having severe sciatic pain and foot drop in my right side. The Neurosurgeon seemed to think it would be an outpatient procedure. Too many years of not taking care of myself has started to catch up.

|
Re: Can’t figure out the triggers September 01, 2018 02:56PM |
Registered: 6 years ago Posts: 18,881 |
Beardman - oh - yeah ...well, too low in the spine.... I was curious to know if the disc issues were higher up and had some impingement in areas of the vagus nerve, but not down there. I certainly wish you every success with the procedure.
There are some specialists in this area that are injecting special forms of what I'll call "collagen" for lack of a better term...into areas to help regenerate discs which are the 'cushions' between the bones of the spine. The results are said to be amazing. I have no personal experience... just hearing from others. You definitely want to get those repaired as minimally invasive as possible...so you can get back to a normal, active life. Keep us posted.
Best to you,
Jackie
There are some specialists in this area that are injecting special forms of what I'll call "collagen" for lack of a better term...into areas to help regenerate discs which are the 'cushions' between the bones of the spine. The results are said to be amazing. I have no personal experience... just hearing from others. You definitely want to get those repaired as minimally invasive as possible...so you can get back to a normal, active life. Keep us posted.
Best to you,
Jackie
|
Re: Can’t figure out the triggers September 01, 2018 03:05PM |
Registered: 5 years ago Posts: 45 |
Quote
Jackie
Beardman - oh - yeah ...well, too low in the spine.... I was curious to know if the disc issues were higher up and had some impingement in areas of the vagus nerve, but not down there. I certainly wish you every success with the procedure.
There are some specialists in this area that are injecting special forms of what I'll call "collagen" for lack of a better term...into areas to help regenerate discs which are the 'cushions' between the bones of the spine. The results are said to be amazing. I have no personal experience... just hearing from others. You definitely want to get those repaired as minimally invasive as possible...so you can get back to a normal, active life. Keep us posted.
Best to you,
Jackie
My cousin is actually a rep for one of those companies. He is sending my MRI around for some opinions. I’m guessing though with the nerve damage (numbness and foot drop) that surgery will be the instant fix that I’m going to need.
|
Re: Can’t figure out the triggers September 06, 2018 09:57AM |
Registered: 5 years ago Posts: 45 |
Just when I thought I was making headway . . .
The decrease in Ca+ seemed to be working wonders. I went 6+ days without a single episode. Unfortunately, that ended for me Tuesday morning while I was sleeping (I have never recorded an episode during sleep before). I have been out of rhythm since then no matter what workout(s) I have tried.
During this 6 day stretch, my resting heart rate was floating around 45 and dropping down to 30-35 during sleep. I was still working out almost every day and I was feeling great!
Any ideas now?
The decrease in Ca+ seemed to be working wonders. I went 6+ days without a single episode. Unfortunately, that ended for me Tuesday morning while I was sleeping (I have never recorded an episode during sleep before). I have been out of rhythm since then no matter what workout(s) I have tried.
During this 6 day stretch, my resting heart rate was floating around 45 and dropping down to 30-35 during sleep. I was still working out almost every day and I was feeling great!
Any ideas now?
|
Re: Can’t figure out the triggers September 06, 2018 11:19AM |
Registered: 6 years ago Posts: 444 |
"Calcium is especially important for athletes because they are more likely to lose calcium, as well as other minerals, through perspiration."
[www.uofmhealth.org]
Edited 1 time(s). Last edit at 09/06/2018 11:20AM by jpeters.
[www.uofmhealth.org]
Edited 1 time(s). Last edit at 09/06/2018 11:20AM by jpeters.
|
Re: Can’t figure out the triggers September 06, 2018 11:48AM |
Registered: 5 years ago Posts: 45 |
Quote
jpeters
"Calcium is especially important for athletes because they are more likely to lose calcium, as well as other minerals, through perspiration."
[www.uofmhealth.org]
Could just be a balance of Ca+, perhaps the weeks I stayed in rhythm was all the Ca+ excess working its way out.
|
Re: Can’t figure out the triggers September 06, 2018 01:09PM |
Registered: 6 years ago Posts: 18,881 |
Beardman - Good you are getting rid of the excess calcium since anytime there is too much intracellular calcium... which is almost always the case with afibbers, there is also the finding that intracellular magnesium is low. The ratios of calcium-to-magnesium and potassium-to-sodium are established by fundamental biophysics... along with the calcium-to- sodium ratio that is often out of balance in those with hypertension.
Low magnesium causes many more health issues than arrhythmia... but like low magnesium causing muscle cramps, it definitely is attention getting.
Keep up the good work.
Jackie
Low magnesium causes many more health issues than arrhythmia... but like low magnesium causing muscle cramps, it definitely is attention getting.
Keep up the good work.
Jackie
|
Re: Can’t figure out the triggers September 06, 2018 01:43PM |
Registered: 5 years ago Posts: 45 |
Quote
Jackie
Beardman - Good you are getting rid of the excess calcium since anytime there is too much intracellular calcium... which is almost always the case with afibbers, there is also the finding that intracellular magnesium is low. The ratios of calcium-to-magnesium and potassium-to-sodium are established by fundamental biophysics... along with the calcium-to- sodium ratio that is often out of balance in those with hypertension.
Low magnesium causes many more health issues than arrhythmia... but like low magnesium causing muscle cramps, it definitely is attention getting.
Keep up the good work.
Jackie
I have noticed a fair amount of muscle cramps lately, but I attributed that to my increase in biking at the gym. I swapped out running because of my back/leg issues for biking.
I do take a magnesium supplement and I also cut way back on my supplements, so maybe something there is off too. I am now taking
Nattokinase (2,000 FU 1x day)
Taurine (1,000mg 3x day)
Hawthorne Extract (300mg 3x day)
Chelated Magnesium Bisglycinate (200mg 2x day)
|
Re: Can’t figure out the triggers September 06, 2018 02:19PM |
Registered: 6 years ago Posts: 444 |
|
Re: Can’t figure out the triggers September 06, 2018 02:50PM |
Registered: 5 years ago Posts: 45 |
Quote
jpeters
I have noticed a fair amount of muscle cramps lately, but I attributed that to my increase in biking at the gym. I swapped out running because of my back/leg issues for biking.
"Without enough calcium you may experience muscle cramps."
Yep, I read through that too. It really is such a fine balancing act.
|
Re: Can’t figure out the triggers September 06, 2018 03:57PM |
Registered: 10 years ago Posts: 1,748 |
Cal. is a no no on this board, I see a Holistic doc. twice a year, Dr. Brownstein. he has written a number of books one of which is "Overcoming Arthritis" he names some of the minerals that is needed and he includes Calcium, he says Calcium is essential to maintain the structural integrity of the body, it is a vital component of strong bones and teeth. Inadequate calcium intake is associated with osteoporosis. He says vit. D levels are necessary for proper absorption of calcium. His recommended dose is 1000-1500 mg. per day of calcium citrate. Of course he includes Magnesium, he says 400 mg. per day. I don't take any cal. supplements but I do eat cheese and it doesn't bother me. We have to do what works for us.
Liz
Liz
|
Re: Can’t figure out the triggers September 06, 2018 04:10PM |
Registered: 6 years ago Posts: 444 |
Consumption connection? Except in certain rare metabolic disturbances that raise blood calcium, calcification of joints and tendons is a local process that's not influenced by calcium intake.
Consumption connection? Many consumer Web sites and even some physicians suggest that people who have had kidney stones should lower their calcium intake to prevent a recurrence. They are incorrect. In fact, dietary calcium actually appears to reduce stone formation.
Consumption connection? Evidence is limited, but calcium intake doesn't appear to increase the risk of calcification in coronary arteries. In fact, a high level of calcium in the diet is usually thought to be beneficial to heart health, because it's associated with lower blood pressure and lower weight
Consumption connection? Calcium intake through diet and supplements is not associated with benign breast calcifications. Moreover, a 2009 study of more than 60,000 Swedish women found that greater calcium intake did not raise the risk of breast cancer.
[www.health.harvard.edu]
Consumption connection? Many consumer Web sites and even some physicians suggest that people who have had kidney stones should lower their calcium intake to prevent a recurrence. They are incorrect. In fact, dietary calcium actually appears to reduce stone formation.
Consumption connection? Evidence is limited, but calcium intake doesn't appear to increase the risk of calcification in coronary arteries. In fact, a high level of calcium in the diet is usually thought to be beneficial to heart health, because it's associated with lower blood pressure and lower weight
Consumption connection? Calcium intake through diet and supplements is not associated with benign breast calcifications. Moreover, a 2009 study of more than 60,000 Swedish women found that greater calcium intake did not raise the risk of breast cancer.
[www.health.harvard.edu]
|
Re: Can’t figure out the triggers September 06, 2018 08:56PM |
Registered: 8 years ago Posts: 1,102 |
Quote
beardman
I have noticed a fair amount of muscle cramps lately, but I attributed that to my increase in biking at the gym. I swapped out running because of my back/leg issues for biking.
I do take a magnesium supplement and I also cut way back on my supplements, so maybe something there is off too. I am now taking
Nattokinase (2,000 FU 1x day)
Taurine (1,000mg 3x day)
Hawthorne Extract (300mg 3x day)
Chelated Magnesium Bisglycinate (200mg 2x day)
How about potassium? I had a hypokalemic paralysis event about 7 years ago and, in hindsight, it was preceded by several weeks of severe muscle pains.
|
Re: Can’t figure out the triggers September 06, 2018 09:21PM |
Registered: 5 years ago Posts: 45 |
Quote
wolfpack
I have noticed a fair amount of muscle cramps lately, but I attributed that to my increase in biking at the gym. I swapped out running because of my back/leg issues for biking.
I do take a magnesium supplement and I also cut way back on my supplements, so maybe something there is off too. I am now taking
Nattokinase (2,000 FU 1x day)
Taurine (1,000mg 3x day)
Hawthorne Extract (300mg 3x day)
Chelated Magnesium Bisglycinate (200mg 2x day)
How about potassium? I had a hypokalemic paralysis event about 7 years ago and, in hindsight, it was preceded by several weeks of severe muscle pains.
Whenever I take potassium it seems to get my heart racing. Generally when I’m out of rhythm I’m around 80bpm, but when I’ve taken potassium it jumps up to 120-130bpm.
|
Re: Can’t figure out the triggers September 09, 2018 09:16AM |
Registered: 6 years ago Posts: 18,881 |
Since this forum is about helping to stabilize and keep hearts calm, it makes sense to understand
the fundamental properties regarding the function of magnesium and calcium.
To recommend taking calcium supplements without knowing intracellular levels of each would be, to put it mildly,
“risky” since that can result in an increase of ectopy or outright arrhythmia – especially if one is already low or
borderline in intracellular magnesium levels..
Calcium is considered to be excitatory, stimulating and responsible for muscle contraction and cellular
electrical excitability. Whereas, magnesium is relaxing. Both are needed, but if the goal is to help
maintain freedom from heart cells firing too frequently or erratically, then it is logical (and smart) to keep
calcium intake at a minimal level; that is, just enough to meet the body’s requirements for the functionality
of electrical and muscle cells… but not enough to induce calcium overload.
The argument that calcium supplements are needed for bone health has long been clarified via the
science of bone morphology stating that calcium is only one mineral component of bone and that an
over-abundance of calcium intake does not insure stronger bones, but rather creates the risk of excess
calcium with overflow storage ending up as arterial calcifications, heart valve calcifications, bone spurs,
and the topic of this post…identifying triggers …that which contributes to the irritation/excitability of
heart cells translating to arrhythmia.
Calcium is typically much easier to acquire from food but magnesium is much more difficult for the quantities
needed to meet all the various requirements of magnesium in the body. .
Cardiologist, Thomas E. Levy, MD, JD, in his book, Death by Calcium, goes into considerable detail
listing the consequence of excess calcium in causing various health problems, most specifically, of
interest to our forum…. that “Excess Calcium Promotes Heart Disease”.. (p. 35) He notes that:
“The real problem is not a lack of calcium in the diet but rather a “relocation of calcium from bones
to other areas of the body”… which he explains and documents with study references.
In the classic book The Magnesium Factor (2003) by magnesium researcher,
the late Mildred S. Seelig, MD, MPH, Chapter 1 is titled “Magnesium: The Mineral that Combats
Heart Disease and Keeps Blood Vessels Healthy”… she correlates the increasing lack of magnesium
from 1900 to nearly 20 years ago when this book was published… showing the increase in heart-
related death and the declining average magnesium intake. One segment, titled:
“Magnesium and Calcium: A Delicate Balance” lists the properties and functions of calcium’s cellular
functions… including these points:
Quote:
Calcium exists mainly outside of cells, whereas almost all magnesium is found inside cels.
Calcium excites nerves, whereas magnesium calms them
Calcium(with potassium) is necessary for muscle contractions; whereas magnesium is
necessary for muscles to relax.
Calcium is necessary for the blood-clotting reaction, which is necessary for wound healing,
whereas magnesium keeps the blood flowing freely and prevents abnormal coagulation within
blood vessels, where clotting reactions could be dangerous.
Calcium is mostly found in bones and gives them much of their hardness, whereas magnesium
is found mainly in soft structure. Bone matrix, the soft structure within bone, contains protein
and magnesium and gives the bones some flexibility and resistance to brittleness.
The normal concentration of magnesium ion inside cells is easily 10,000 times that of intracellular
Calcium ions – under healthy conditions. But if the amount of magnesium in a cell falls, for any reason,
Calcium flows into the cell. With this abnormal situation, this happens:
1. Higher than normal calcium inside a cell excites a lot of reactions. It puts the cell into a hyperactive state. Heart and blood-vessel cells are especially excitable because they need to react rapidly during sudden stress situation.
As such they are truly vulnerable to deficits in magnesium that allow abnormal rises in calcium, with resulting hyperactivity. end quote
(pp 14 , 15).
While it’s not new news, how many of us who visited our family doctor or consulted a cardiologist when we first began having palpitations or arrhythmia, had the doctor say… “let’s test you for magnesium?” Chances are, virtually none… and even if we had, it would have been serum magnesium (from a blood draw) which wouldn’t have detected the low intracellular Mg status which was undoubtedly present. Observations back in the 80's....
1980 study - Serum magnesium in acute myocardial infarction. Relation to arrhythmias.
[www.ncbi.nlm.nih.gov]
1981 study Relation between potassium, magnesium and cardiac arrhythmias.
[www.ncbi.nlm.nih.gov]
1986 study Magnesium and potassium. Inter-relationships in cardiac disorders.
[www.ncbi.nlm.nih.gov]
Just keep in mind that magnesium repletion is a very fluid status and you have to keep working at optimizing the IC stores continually.... it may take months to reach that level...and some people never do because of so many influencing factors that deplete Mg quickly.... stress being high on the list. Physical, endurance exercise is stress.
The other rule is… if you are low in IC Mg, adding potassium before Mg optimization will most always result in ectopics and/or arrhythmia.
Jackie
the fundamental properties regarding the function of magnesium and calcium.
To recommend taking calcium supplements without knowing intracellular levels of each would be, to put it mildly,
“risky” since that can result in an increase of ectopy or outright arrhythmia – especially if one is already low or
borderline in intracellular magnesium levels..
Calcium is considered to be excitatory, stimulating and responsible for muscle contraction and cellular
electrical excitability. Whereas, magnesium is relaxing. Both are needed, but if the goal is to help
maintain freedom from heart cells firing too frequently or erratically, then it is logical (and smart) to keep
calcium intake at a minimal level; that is, just enough to meet the body’s requirements for the functionality
of electrical and muscle cells… but not enough to induce calcium overload.
The argument that calcium supplements are needed for bone health has long been clarified via the
science of bone morphology stating that calcium is only one mineral component of bone and that an
over-abundance of calcium intake does not insure stronger bones, but rather creates the risk of excess
calcium with overflow storage ending up as arterial calcifications, heart valve calcifications, bone spurs,
and the topic of this post…identifying triggers …that which contributes to the irritation/excitability of
heart cells translating to arrhythmia.
Calcium is typically much easier to acquire from food but magnesium is much more difficult for the quantities
needed to meet all the various requirements of magnesium in the body. .
Cardiologist, Thomas E. Levy, MD, JD, in his book, Death by Calcium, goes into considerable detail
listing the consequence of excess calcium in causing various health problems, most specifically, of
interest to our forum…. that “Excess Calcium Promotes Heart Disease”.. (p. 35) He notes that:
“The real problem is not a lack of calcium in the diet but rather a “relocation of calcium from bones
to other areas of the body”… which he explains and documents with study references.
In the classic book The Magnesium Factor (2003) by magnesium researcher,
the late Mildred S. Seelig, MD, MPH, Chapter 1 is titled “Magnesium: The Mineral that Combats
Heart Disease and Keeps Blood Vessels Healthy”… she correlates the increasing lack of magnesium
from 1900 to nearly 20 years ago when this book was published… showing the increase in heart-
related death and the declining average magnesium intake. One segment, titled:
“Magnesium and Calcium: A Delicate Balance” lists the properties and functions of calcium’s cellular
functions… including these points:
Quote:
Calcium exists mainly outside of cells, whereas almost all magnesium is found inside cels.
Calcium excites nerves, whereas magnesium calms them
Calcium(with potassium) is necessary for muscle contractions; whereas magnesium is
necessary for muscles to relax.
Calcium is necessary for the blood-clotting reaction, which is necessary for wound healing,
whereas magnesium keeps the blood flowing freely and prevents abnormal coagulation within
blood vessels, where clotting reactions could be dangerous.
Calcium is mostly found in bones and gives them much of their hardness, whereas magnesium
is found mainly in soft structure. Bone matrix, the soft structure within bone, contains protein
and magnesium and gives the bones some flexibility and resistance to brittleness.
The normal concentration of magnesium ion inside cells is easily 10,000 times that of intracellular
Calcium ions – under healthy conditions. But if the amount of magnesium in a cell falls, for any reason,
Calcium flows into the cell. With this abnormal situation, this happens:
1. Higher than normal calcium inside a cell excites a lot of reactions. It puts the cell into a hyperactive state. Heart and blood-vessel cells are especially excitable because they need to react rapidly during sudden stress situation.
As such they are truly vulnerable to deficits in magnesium that allow abnormal rises in calcium, with resulting hyperactivity. end quote
(pp 14 , 15).
While it’s not new news, how many of us who visited our family doctor or consulted a cardiologist when we first began having palpitations or arrhythmia, had the doctor say… “let’s test you for magnesium?” Chances are, virtually none… and even if we had, it would have been serum magnesium (from a blood draw) which wouldn’t have detected the low intracellular Mg status which was undoubtedly present. Observations back in the 80's....
1980 study - Serum magnesium in acute myocardial infarction. Relation to arrhythmias.
[www.ncbi.nlm.nih.gov]
1981 study Relation between potassium, magnesium and cardiac arrhythmias.
[www.ncbi.nlm.nih.gov]
1986 study Magnesium and potassium. Inter-relationships in cardiac disorders.
[www.ncbi.nlm.nih.gov]
Just keep in mind that magnesium repletion is a very fluid status and you have to keep working at optimizing the IC stores continually.... it may take months to reach that level...and some people never do because of so many influencing factors that deplete Mg quickly.... stress being high on the list. Physical, endurance exercise is stress.
The other rule is… if you are low in IC Mg, adding potassium before Mg optimization will most always result in ectopics and/or arrhythmia.
Jackie
|
Re: Can’t figure out the triggers September 19, 2018 06:25PM |
Registered: 5 years ago Posts: 45 |
I’m still working on getting my mg levels up, currently at 600mg daily. I am wondering how much others are able to take. Also, are topical magnesium sprays any use to us afibbers?
My in and out of rhythm cycles seem to be extending. I was in rhythm for 6 days, but then out for 8. I was then in NSR for the last 8 days, but I think I pushed my workout too hard last night. I felt off last night although I was still registering NSR on my s Kardia. When I woke up this morning I was out and looking at my HR it happened at around 2:00, 2 hours after going to sleep. Fingers crossed on converting fast as that 8 day stint out of rhythm was a killer.
Edited 1 time(s). Last edit at 09/19/2018 07:03PM by beardman.
My in and out of rhythm cycles seem to be extending. I was in rhythm for 6 days, but then out for 8. I was then in NSR for the last 8 days, but I think I pushed my workout too hard last night. I felt off last night although I was still registering NSR on my s Kardia. When I woke up this morning I was out and looking at my HR it happened at around 2:00, 2 hours after going to sleep. Fingers crossed on converting fast as that 8 day stint out of rhythm was a killer.
Edited 1 time(s). Last edit at 09/19/2018 07:03PM by beardman.
|
Re: Can’t figure out the triggers September 06, 2019 03:21PM |
Registered: 7 years ago Posts: 218 |
|
Re: Can’t figure out the triggers September 07, 2019 09:05AM |
Registered: 5 years ago Posts: 45 |
Quote
hwkmn05
Cardiologist, Thomas E. Levy, MD, JD, in his book, Death by Calcium
Another great read by Dr. Thomas Levy is "Hidden Epidemic". A personal story of his own root canal teeth he believed to be the direct cause for his heart attack and other health issues until removal.
Thank you for the reply, I’ll check those out.
I’m about 1.5 years post diagnosis and finally decided to go on the flecainide and Metoprolol. I honestly just couldn’t take the mental hot anymore. No matter what I tried, it seemed I couldn’t stay in rhythm more that 50% of the time. The echocardiogram from 1.5 years ago to now show zero difference so it would appear that it was still not effecting me physically.
I have noticed though a significant weight gain since taking the meds. I was on 100mg flecainide 2x daily and 50mg metoprolol 2x daily. That wasn’t keeping it quite in check so they bumped the flecainide up to 150mg which has now been working for a few months.
I also moved across the country so now I have to find a new cardiologist. Any insight on the weight gain on these meds? I’ve picked up about 30lbs with no change in diet or exercise routine.
Thank you in advance
Sorry, only registered users may post in this forum.